Translate this page into:
Uphill battle: The saga of hCG research that led to a paradigm shift
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Human chorionic gonadotropin (hCG), is a heterodimeric glycoprotein, primarily produced and secreted by placental syncytiotrophoblasts in large quantities. Some normal and cancer tissues can also secrete hCG in small quantities but it is short lived in the circulation due to lower abundance of carbohydrate moieties on the hCG molecules1. Placental hCG is a collection of molecules differing in structure, function and circulatory half-lives. The hCG is also present in subhuman primates, but not in other animal species1. It not only belongs to glycoprotein hormones family, but also to the cystine knot growth factor family, which consists of transforming growth factors-ß, platelet derived growth factor and nerve growth factor. Belonging to the same family implies that these diverse set of molecules may have some common functional features.
hCG is structurally and functionally similar to luteinizing hormone (LH), secreted by gonadotropes in anterior pituitary gland. Because there is only one receptor, hCG and LH mimic each other's functions2. However, these functions differ quantitatively, which primarily arise from the differences in their circulatory half-lives. hCG has a longer circulatory half-life than LH, due to abundance of carbohydrate residues. It is theoretically possible however, that hCG and LH may have distinct functions in select tissues and situations, due to potential unique conformational changes that each hormone can induce in the same receptor molecules. The LH is present in circulation in a cyclical manner during non-pregnancy and once pregnancy is initiated, the cyclicity stops and the levels fall to base-line and remain there until menstrual cycles resume after lactation.
Although hCG presence is restricted to humans and subhuman primates, but LH is present in all species. Unicellular organisms, fish and nematodes also contain structurally similar CG and/or LH molecules, but their functions may not necessarily be the same345. It has been a mystery for decades why only humans and subhuman primates have hCG, when they already have a functionally similar LH6. The best guess is that evolutionary and selection pressures may have led to the CG appearance. These pressures could have been that human and primate pregnancies might have faced unusual hurdles during evolution and to overcome them, sturdier, longer lasting and multifunctional molecule such as CG, might have been required78. The CG appearance required its receptors and signaling systems and all three might have co-evolved. Different hormone receptor systems share the same signaling systems. This sharing might have been made possible by an evolution of co-regulatory molecules, which allowed for specificity, sensitivity and additional sites of regulation.
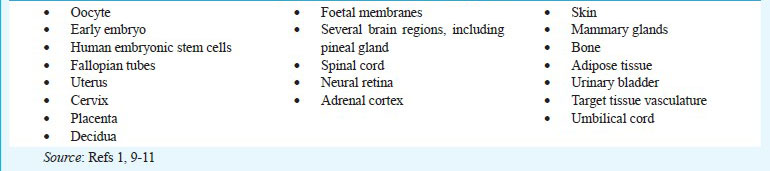
The identification of hCG dates back more than 50 years. Most of that time, it was known for its actions to rescue corpus luteum from regression in a fertile cycle. Corpus luteum is needed for secretion of progesterone, which maintains pregnancy. The progesterone secretion progressively shifts from corpus luteum to placenta and is completed by about the 9th week of pregnancy. This completion obviates the need for the corpus luteum for pregnancy continuation. However, both the corpus luteum and hCG are maintained throughout pregnancy. It does not make sense for cells to continue secreting hCG, when it has no function during the remainder of the pregnancy. The chances are that hCG has other functions. Indeed, the research in the past 25 yr has shed light on this possibility. It is now known that many other tissues respond to hCG191011 (Box).
The hCG actions in these tissues is context, tissue and cell type dependent91011. The sum of all the hCG actions during pregnancy can be summarized into five categories: those that favour pregnancy initiation, pregnancy maintenance, safeguard foetus from rejection, support foetal growth and development and allow delivery when foetus is sufficiently mature so it can survive outside the womb. The probable evolutionary significance of hCG actions is to safeguard pregnancy against all the odds during the evolution of primates. This could also include providing a relief from maladies that could potentially interfere with the successful completion of pregnancy. These maladies, for example, could be rheumatoid arthritis, certain pathogen infections and other conditions which threaten pregnancy continuation. In view of the above discussion, it is easy to understand why hCG has such broad regulatory roles in the body.
This leads to the next issue of whether the broad regulatory roles of hCG are totally unexpected. The answer is simply no. As it turns out that many other hormones, for example, prolactin, follicle stimulating hormone (FSH), gonadotropin releasing hormone, oxytocin, relaxin, etc. have multiple sites of action beyond their conventional targets and there is no reason that hCG should be any different from these other hormones. The multiple uses of hormones may have been conserved because of the environment and mode of life changes during the evolution of organisms. Finally, multiple hormone uses could represent a functional redundancy and efficiency.
The finding that hCG regulates multiple target tissues, represents a paradigm shift. This paradigm shift has offered likely explanations for many poorly understood things about human pregnancy such as, why breast cancer risk decreases in women who complete a full term pregnancy before 20 yr of age, why pregnancy ameliorates the symptoms of rheumatoid arthritis, whether there is an hormonal basis for behavioural changes and urinary tract symptoms seen during pregnancy and why foetus is not often infected when mother is HIV positive. There is also a pathological relevance for the paradigm shift. For example, gestational trophoblastic diseases, hyperemesis gravidarum, several pregnancy complications, etc can now be attributed to some of the facet of hCG actions. Paradigm shift offered likely explanations for some of the age related health issues, such as endometrial cancer, osteoporosis, Alzheimer's disease, etc.1011.
The paradigm shift offered the novel therapeutic options, such as treatment of miscarriages, preterm birth, breast cancer, gynaecological infections, HIV/AIDS and rheumatoid arthritis. These potential novel therapies with hCG are inexpensive, non-toxic, have minimal or no side effects and no harm is likely in case of treatment failure.
References
- Endocrinology of the trophoblast tissue. In: Becker K, ed. Principles and practice of endocrinology and metabolism (3rd ed). Philadelphia, PA: Lippincott Williams & Wilkins; 2001. p. :1096-102.
- [Google Scholar]
- Knockout of gonadotropins and their receptor genes. In: Henry HL, Norman AW, eds. Encyclopedia of hormones, Simpson E, Section, editor. Female reproduction. San Diego, California: Academic Press; 2003. p. :554-6.
- [Google Scholar]
- Functional divergence of glycoprotein hormone receptors. Integr Comp Biol. 2010;50:110-23.
- [Google Scholar]
- The pregnancy hormones human chorionic gonadotropin and progesterone induce human embryonic stem cell proliferation and differentiation into neuroctodermal rosettes. Stem Cell Res Therapy. 2010;1:1-13.
- [Google Scholar]
- Evolution of glycoprotein hormone subunit genes in bilateral metazoa: identification of two novel human glycoprotein hormone subunit family genes, GPA2 and GPB5. Mol Endocrinol. 2002;16:1538-51.
- [Google Scholar]
- Chorionic gonadotropin has a recent origin within primates and an evolutionary history of selection. Mol Biol Evol. 2002;19:320-35.
- [Google Scholar]
- Nongonadal actions of LH and hCG in reproductive biology and medicine. Semin Reprod Med. 2001;19:1-119.
- [Google Scholar]
- The past, present and future of nongonadal LH/hCG actions in reproductive biology and medicine. Mol Cell Endocrinol. 2007;269:2-8.
- [Google Scholar]
- Recent progress in luteinizing hormone/human chorionic gonadotropin hormone research. Mol Hum Reprod. 2009;15:703-11.
- [Google Scholar]




