Translate this page into:
Clinical & immunological profile of newly diagnosed patients with youth onset diabetes mellitus
Reprint requests: Dr Dinesh K. Dhanwal, Director Professor of Medicine & Endocrinologist, Maulana Azad Medical College, New Delhi 110 002, India e-mail: dineshdhanwal@hotmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
There has been a rise in the incidence of diabetes mellitus in the younger population of India. There are limited data available on the immunological profile of youth onset diabetes mellitus (DM) especially in type 2. Therefore, this study was undertaken to evaluate the clinical and immunological profile of youth onset DM in north India.
Methods:
Fifty one consecutive patients of 8-35 yr of age with diabetes mellitus attending the Lok Nayak Hospital, Maulana Azad Medical College, New Delhi, and Hormone Care and Research Center at Ghaziabad, Uttar Pradesh, India, were included in the study. All subjects were tested for glutamic acid decarboxylase (GAD), an islet cell antigen ICA512/IA2, and insulin antibodies. GAD and ICA512/IA2 were done by ELISA and insulin autoantibodies were tested by radioimmunoassay (RIA) method. These patients were also screened for hepatitis A to E, cytomegalovirus (CMV) and Epstein-Barr virus (EBV) as trigger factors for onset of type 1 DM.
Results:
Of the total 51 patients, 38 were men and 13 were women. The mean age and BMI of the subjects was 19.7 (±7) years and 21 (± 5) kg/m2, respectively. Twenty patients were below the age of 18 yr and their height was more than 75th percentile of Indian standards. All patients were symptomatic and 12 of these presented with ketoacidosis. Only 48 per cent (n=24) were positive for GAD, 14 per cent (n=7) for ICA512/IA-2, and 28% (n=14) were positive for insulin antibody. Five of these patients had evidence of hepatitis E virus infection. None of the subjects had evidence of active CMV or EBV infection.
Interpretation & conclusions:
About half of the youth onset diabetes mellitus patients from north India had presence of pancreatic autoimmunity in the form of GAD, ICA512/IA2, and insulin antibodies or a combination of antibodies suggestive of having type 1 DM. Further studies need to be done on a large sample size in different parts of the country.
Keywords
Anti-GAD antibody
HbAlc
pancreatic auto antibodies
type 1 diabetes mellitus
youth onset diabetes

The prevalence of diabetes mellitus (DM) is increasing throughout the world, especially in developing countries, including India due to changing lifestyles of people and genetic background. Diabetes is disproportionately higher in the young adult population in Asian countries unlike in the West, where it is more common in older people. In 2012, 371 million people in the age group 20-79 yr were suffering from diabetes with China having maximum number followed by India1. It will cause great economic burden on health resources worldwide especially in developing countries2. Diabetes in India including in younger population (<25 yr) is an alarming situation because of its economic and social impact on society23. Studies from India and the USA have shown increased prevalence of diabetes in younger population45. In India, 10 per cent of diagnosed patients with diabetes were less than 30 yr of age in 20026. The types of diabetes in the youth population from India was classified in to classical type 1, classical type 2, ketosis resistant youth diabetes, pancreatic diabetes or maturity onset diabetes mellitus7. The diagnosis and classification of diabetes are based on the clinical and immunological profile of the patients. Immunological markers, such as the pancreatic islet cell antibodies, including insulin antibodies, anti-GAD, (glutamic acid decarboxylase), and anti-ICA512/IA2, an islet cell antigen are used for differentiation between different types of diabetes in the younger population. Earlier studies have reported clinical profile and variable percentages of antibody positivity in youth onset diabetes mellitus from South Asia891011121314. However, none of these studies has reported all three antibodies together in youth onset diabetes mellitus in India. Genetic background predisposes a person to type 1 DM15. However, a trigger factor is required for the onset of diabetes. The most common trigger factor is a viral infection16. There is a paucity of data on the trigger factor for onset of type 1 diabetic from India. Therefore, the present study was aimed to evaluate clinical and immunological profile of patients with youth onset diabetes mellitus patients from north India.
Material & Methods
The study subjects were part of the Protégé Encore study, a phase 3, randomized, double blind, multinational, placebo controlled study to evaluate efficacy and safety of Teplizumab (MGA031), a humanized, anti-CD3 monoclonal antibody, in children and adults with recent onset type 1 diabetes mellitus17. The study population in this sub study was selected from Maulana Azad Medical College associated Lok Nayak Hospital, New Delhi, and Hormone Care and Research Center, Ghaziabad, Uttar Pradesh, India. The recruitment period was from January to July 2010 and sample size was based on the number of patients screened at these two centers. Participants were eligible if they met the following criteria: aged 8-35 yr; body mass of at least 36 kg; type 1 diabetes mellitus diagnosed for 12 wk or less, with need for injected insulin therapy; detectable fasting or stimulated C-peptide; and positive autoantibody titre against an islet-cell antigen (ICA-512/IA-2), glutamic acid decarboxylase (GAD 65), or insulin, within 2 wk of initiating insulin treatment. Exclusion criteria focused on medical disorders that would potentially confound results or interfere with safe completion of the trial, including serious cardiovascular disorders, active infections, and recent participation in a clinical trial, vaccination, or pregnancy. Criteria for diagnosis of diabetes were as per standard American Diabetes Association (ADA) guidelines18.
All study patients were subjected to clinical and biochemical tests as per pre-designed case record form. The laboratory tests included complete blood count, blood glucose levels, kidney and liver function tests, lipid profile, HbA1c, and urine for micro-HbA1c albumin. Immunological profile included detection of antibodies against glutamic acid decarboxylase (GAD Ab), a tyrosine phosphatase-like protein (ICA 512/IA-2 Ab) and insulin by ELISA method and insulin antibodies were done by radioimmunoassay (RIA) method from kits supplied by Kronus (Boise, USA). The levels of three autoantibodies were measured in a licensed central laboratory (Quintiles Laboratories, Singapore). The cut-off values for GAD Ab, ICA512/IA-2 and insulin antibodies were 5 IU/ml, 15 and 0.4 U/ml, respectively. All three kits were tested for performance qualification before study sample analysis. Calibration verification, sensitivity, precision, and dilution verification were evaluated. The immunological profile for anti-GAD, anti-ICA512/IA-2 and anti-insulin antibodies was done in all patients. The patients having antibodies alone or combination were considered as suffering from type 1 DM and the remaining patients were classified as type 2 DM.
Further, all patients were tested for active viral infections such as, hepatitis A-E, cytomegalovirus (CMV), and Epstein-Barr virus (EBV) by antigen detection methods. Hepatitis A antibody total (anti-HAV total) and hepatitis A IgM antibody (anti-HAV, IgM) were tested by Bayer Chemiluminescence. Qualitative immunoassay was used for the hepatitis screen panel (HBsAg, anti-HCV). Hepatitis B surface antigen (HBsAg) confirmation was tested by Bayer Chemiluminescence. HCV RIBA was done by National University Hospital (Singapore). Diasorin EIA (enzyme immunoassay) was used for hepatitis D (Delta) antibody (anti-D) detection and hepatitis E IgG antibodies were done by Metropolis (Mumbai, India). Epstein-Barr virus and CMV were tested using polymerase chain reaction (PCR). IgM and IgG antibodies for EBV and IgG antibodies for CMV were tested in all patients by EIA and immunoflourescence, respectively. Institutional ethics committee approved the study protocol, and all participants or guardians gave written informed consent.
Statistical analysis: Data were analyzed using SSPS for windows 10. Statistical methods used were descriptive to calculate mean ± SD.
Results
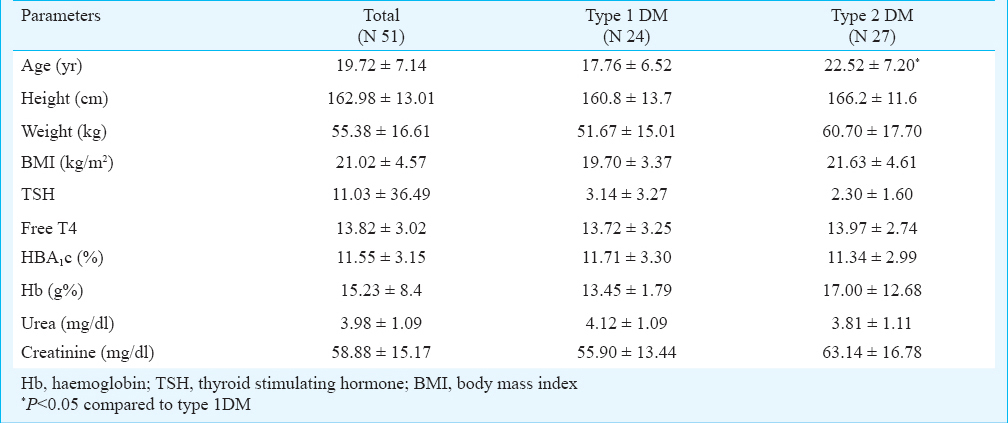
The baseline characteristics of subjects are given in the Table. Of the total 51 subjects, 38 were men and 13 were women. The mean age was 19.72±7.14 yr, and BMI was 21.02±4.57 kg/m2. Twenty subjects were below the age 18 and their height was more than 75th percentile of Indian standards. Eleven subjects who were less than 18 yr of age had a height of >75 % percentile as per Indian growth charts. There was no significant difference in different parameters in type 1 and type 2 subjects except the age was significantly (P<0.05) higher in type 2 group. All subjects were symptomatic for diabetes and 12 of these patients presented with ketoacidosis at the time of diagnosis. The remaining patients presented with osmotic symptoms. There was no sign of neuropathy, retinopathy, and nephropathy in these patients at the time of inclusion. Mean HbA1c level of all patients was 11.55 per cent. All patients had normal blood counts, lipid profile, and kidney and liver function tests. Mean thyroid stimulating hormone (TSH) level was 11.03±36.49 uIU/ml. Only 12 per cent patients had hypothyroidism.
Anti-GAD Ab was present in 24 (48%) patients. ICA512/IA2 antibody was detected in seven (14%) patients, and 14 (28%) patients had insulin antibodies. Seven (14%) patients showed presence of both anti-GAD and anti-ICA512/IA2 antibodies and five (9%) patients had both anti-GAD and insulin antibodies. Presence of all three pancreatic antibodies was observed in only three patients.
Antibody-positive patients were younger, had a lower weight and BMI, and most of them presented with diabetic ketoacidosis. There was evidence of active hepatitis E (IgM antibody positive) infection in five patients. None of the patients showed evidence of active CMV, EBV infection or other hepatitis infection.
Discussion
The differentiation between T1DM and T2DM is difficult in young patients but can be done by immunological markers, such as anti-GAD, ICA512/IA2, and insulin antibodies19. In our study, anti-GAD antibodies were present in 48 per cent patients, ICA512/IA2 antibody in 14 per cent and insulin antibody in 28 per cent cases of youth onset diabetes. Further, active viral infection, especially HEV as a possible trigger factor for onset of T1DM was observed in only 10 per cent of cases.
Autoimmunity in youth onset has been reported earlier from India and elsewhere111213. The level of autoimmunity reported in the present study was among the highest reported so far compared to other Indian studies789. Kouchipillai et al6 have shown 38 per cent anti-GAD positivity in their study. However, Pan et al20 reported prevalence as low as 9 per cent in South Indian patients13. A study from north India has shown higher values, i.e. 70 per cent of GAD positivity and 20-26 per cent positivity of ICA antibody in type1diabetic patients20. Goswami et al7 have reported 24.2 per cent pancreatic antibody in youth onset diabetes patients from north India. Other studies such as by Tica et al21 and Thai et al22 have reported 27 and 39.6 per cent positivity of anti-GAD, respectively. Lan et al23 reported 54.6 per cent positivity for anti-GAD and 24 per cent for both anti-GAD and ICA512/IA2 antibodies. Presence of all three antibodies was observed in only three patients. None of the studies have analyzed all antibodies together for diagnosis of type1diabetes. In our study, anti-GAD antibody was present in all antibody positive youth onset DM. Therefore, testing for anti-GAD Ab alone may perhaps suffice as a diagnostic tool in youth onset DM.
Another interesting fact in our study was that five patients of type 1 DM had evidence of active HEV infection. None of the patients showed evidence of recent EBV and CMV virus infections. There are at least two different pathogenic mechanisms in virus-induced diabetes: cytolytic infection of beta cells leading to their destruction, and triggering of autoimmunity leading to the autoimmune-mediated destruction of beta cells24. At least 10 viruses have been implicated as triggering factors in the onset of T1DM. Retrovirus, mumps virus, rubella virus, CMV, enterovirus and EBV are responsible for autoimmune-mediated destruction of beta cells. Other viral infections such as encephalomyocarditis virus, Coxsackie B viruses can lead to direct damage to beta cell2526272829. In our study, only five patients had evidence of HEV infection suggesting its possible role in onset of autoimmune DM in youth. Hepatitis C virus infection has been shown to have a role in the development of T1DM3031. However, another study did not find any correlation between any of the viral hepatitis infections and onset of DM32.
In this study the height of T1DM patients was more than 75 per cent percentile of Indian standard. The increase in height may be attributed to autoimmune phenomenon functioning in growth acceleration as well as production in antibodies in T1DM33.
Our study had certain limitations. We have not done HLA-typing in this study. Further, there was a selection bias as we excluded subjects with signs of insulin resistance.
In conclusion, the presence of pancreatic antibodies was seen among half of the youth onset diabetic patients from north India, anti-GAD Ab being the most common. Similar studies should be done in other parts of the country with a large sample size.
References
- IDF Diabetes Atlas, update 2012. International Diabetes Federation. available from: http://www.idf.org/diabetesatlas/5e/Update2012
- [Google Scholar]
- Current status of diabetes in India and need for novel therapeutic agents. J Assoc Physicians India. 2010;58:7-9.
- [Google Scholar]
- Prevalence of diabetes and prediabetes (impaired fasting glucose and/or impaired glucose tolerance) in urban and rural India: phase I results of the Indian Council of Medical Research-INdia DIABetes (ICMR-INDIAB) study. Diabetologia. 2011;54:3022-7.
- [Google Scholar]
- Age-specific prevalence and risk associations for impaired glucose tolerance in urban southern Indian population. J Assoc Physicians India. 2003;51:766-9.
- [Google Scholar]
- Prevalence of diabetes in U.S. youth in 2009: the SEARCH for diabetes in youth study. Diabetes Care. 2014;37:402-8.
- [Google Scholar]
- Youth-onset diabetes in India: nature of diabetes and use of bovine insulin in their treatment. 2002. RSSDI textbook of diabetes. Available from: www.iddtindia.org/youth.asp
- [Google Scholar]
- Islet cell autoimmunity in youth onset diabetes mellitus in Northern India. Diabetes Res Clin Pract. 2001;53:47-54.
- [Google Scholar]
- Demographic, breast-feeding, and nutritional trends among children with type 1 diabetes mellitus. Indian J Endocrinol Metab. 2011;15:38-42.
- [Google Scholar]
- Clinical and biochemical profiles of young diabetics in North-Eastern India. J Assoc Physicians India. 2002;50:1130-4.
- [Google Scholar]
- Diabetes mellitus among young adults in Sri Lanka-role of GAD antibodies in classification and treatment: The Sri Lanka Young Diabetes study. Diabetologia. 2008;51:1368-74.
- [Google Scholar]
- Clinical profile of diabetes in the young seen between 1992 and 2009 at a specialist diabetes centre in south India. Prim Care Diabetes. 2011;5:223-9.
- [Google Scholar]
- Islet autoimmunity status in Asians with young-onset diabetes (12-40 years): association with clinical characteristics, beta cell function and cardio-metabolic risk factors. Diabetes Res Clin Pract. 2008;80:224-30.
- [Google Scholar]
- Type 1 diabetes versus type 2 diabetes with onset in persons younger than 20 years of age. Ann N Y Acad Sci. 2008;1150:239-44.
- [Google Scholar]
- Antibodies to pancreatic islet cell antigens in diabetes seen in Southern India with particular reference to fibrocalculous pancreatic diabetes. Diabet Med. 1998;15:156-9.
- [Google Scholar]
- Biomarkers of susceptibility to type 1 diabetes with special reference to the Indian population. Indian J Med Res. 2007;125:321-44.
- [Google Scholar]
- Protégé Trial Investigators. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet. 2011;378:487-97.
- [Google Scholar]
- Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 1997;20:1183-97.
- [Google Scholar]
- Metabolic, immunological and clinical characteristics in newly diagnosed Asian diabetes patients aged 12-40 years. Diabet Med. 2004;21:1007-13.
- [Google Scholar]
- Biomarkers of susceptibility to type 1 diabetes with special reference to the Indian population. Indian J Med Res. 2007;125:321-44.
- [Google Scholar]
- Frequency of latent autoimmune diabetes in adults in Asian patients diagnosed as type 2diabetes inet al. Metabolic, immunological and clinical characteristics in newly diagnosed Asi Birmingham, United Kingdom. Ann N Y Acad Sci. 2003;1005:356-8.
- [Google Scholar]
- Anti-GAD antibodies in Chinese patients with youth and adult-onset IDDM and NIDDM. Diabetologia. 1997;40:1425-30.
- [Google Scholar]
- IA-2, a transmembrane protein of the protein tyrosine phosphatase family, is a major autoantigen in insulin-dependent diabetes mellitus. Proc Natl Acad Sci USA. 1996;93:6367-70.
- [Google Scholar]
- Viruses as a triggering factor of type 1 diabetes and genetic markers related to the susceptibility to the virus-associated diabetes. Diabetes Res Clin Pract. 1989;7(Suppl 1):S47-58.
- [Google Scholar]
- Enterovirus infections are associated with the induction of beta-cell autoimmunity in a prospective birth cohort study. J Med Virol. 2003;69:91-8.
- [Google Scholar]
- Enterovirus infection as a risk factor for β-cell autoimmunity in a prospectively observed birth cohort: The Finnish Diabetes Prediction and Prevention Study. Diabetes. 2000;49:1314-8.
- [Google Scholar]
- Mechanisms of coxsackievirus-induced damage to human pancreatic beta-cells. J Clin Endocrinol Metab. 2000;85:432-40.
- [Google Scholar]
- Rotavirus infections and development of diabetes-associated autoantibodies during the first 2 years of life. Clin Exp Immunol. 2002;128:511-5.
- [Google Scholar]
- Hepatitis C virus infection-related Type 1 diabetes mellitus. Diabet Med. 2005;22:340-3.
- [Google Scholar]
- A case of chronic hepatitis C developing insulin-dependent diabetes mellitus associated with various autoantibodies during interferon therapy. Diabetes Res Clin Pract. 2000;49:101-6.
- [Google Scholar]
- Prevalence of hepatitis A, B, C and E virus in adolescents with type-1 diabetes mellitus. Int J Adolesc Med Health. 2003;15:133-7.
- [Google Scholar]
- Height at diagnosis of insulin dependent diabetes in patients and their non-diabetic family members. Br Med J (Clin Res Ed). 1986;292:1419-22.
- [Google Scholar]




