Translate this page into:
Presence of diabetes mellitus in the ‘Dawoodi Bohra youth community’ in Udaipur, Rajasthan
Reprint requests: Dr Shuchi Goyal, Associate Professor, Department of Biochemistry, RNT Medical College Udaipur 313 001, India e-mail: ggoyal0207@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Diabetes mellitus is a major public health problem worldwide. With the rising incidence of diabetes in India, it becomes particularly relevant to ascertain its prevalence in various ethnic groups. The objective of this study was to find out the presence of diabetes mellitus in the ‘Dawoodi Bohra Youth Community’ and also to assess the factors responsible for it.
Methods:
A house-to-house study was conducted and 2179 subjects were questioned randomly; children below 18 yr of age were excluded. A questionnaire was given to each member and questions were also asked to test their level of awareness regarding diabetes which was graded on a 5-pointer scale where 1 meant ‘very poor’ and 5-’excellent’. Diabetes was diagnosed using GOD-POD (oxidase-peroxidase) method according to the WHO criteria.
Results:
Total number of diabetic subjects found was 246 (11.29%) with a mean age of 60.21±10.91 years. The condition was more common in males (58.94%). The highest prevalence was recorded in the age group of 65-69 yr (22.01%) and none had diabetes in the age group 11-24 yr. Pedigree analysis showed that 109 (44.30%) subjects had at least one affected relative and 23 (9.34%) had at least two diabetic family members; 52 were found to have parents with diabetes. On the 5-pointer scale, the overall care in diabetic subjects was 3.76±0.56 as compared to 2.86±0.60 in non-diabetic subjects (P<0.001).
Interpretation & conclusions:
Our results indicated that the marital alliances, familial aggregation and lifestyle could be the major factors which enhanced the chances of diabetes in this community. This research work also reflected poor awareness among these people regarding their health and diseases.
Keywords
Awareness
diabetes
ethnic
prevalence

Diabetes mellitus (DM), is a major public health problem worldwide. In the last two decades, type 2 DM is on the rise1, the degree of which differs between countries and among different ethnic groups within the individual country2.
The World Health Organization (WHO) considers it to be a non-communicable epidemic and has projected that the global prevalence of type 2 DM will be more than double from 135 million in 1995 to 300 million by 20253.
The increasing prevalence of this disease in the modern world has been attributed to an unmasking of genetic defects45 by environmental factors6 brought about by changes in the lifestyle17. Ethnology and social attributes are also important risk factors8. Individual predisposition to type 2 diabetes mellitus is governed by multiple factors but inherited factors seem predominant9. With the rising incidence of diabetes in India it becomes particularly relevant to ascertain its prevalence in various ethnic groups with different cultural and lifestyle practices1.
The ‘Dawoodi Bohra youth community’ is a distinct subgroup amongst the Muslims and comprises approximately one million members worldwide. There are high incidences of consanguineous marriages in this community which help in understanding genetic linkage in the transmission of this disease. No research work on prevalence or familial aggregation of diabetes and transmission patterns of the disease in this community has been reported earlier.
This cross-sectional study was undertaken to determine the presence of diabetes mellitus in the ‘Dawoodi Bohra youth community’ in Udaipur, Rajasthan, India, to assess the social or genetic factors responsible for its high incidence. The study was also aimed to find the level of awareness among people regarding their health.
Material & Methods
This study was conducted in the department of Biochemistry, RNT Medical College, Udaipur, Rajasthan.
A house-to-house study was conducted in the city of Udaipur from April to June 2011. The total population of ‘Dawoodi Bohra youth community’ in this region is approximately 4000 and majority of them reside in Bohrawadi and Kharol Colony (Fatehpura) in Udaipur. The total number of households was approximately 900, of which 505 households were covered and 2179 subjects were questioned eventually. The inclusion criterion was that the person questioned should belong to ‘Dawoodi Bohra youth community’ and children below 18 yr of age were excluded.
So about 50 per cent of the community was randomly surveyed. Diabetes was diagnosed according to World Health Organization Criteria10 in the Central Laboratory where Glucose Oxidase-peroxidase (GOD-POD) (oxidase- peroxidase) method11 was used for estimating blood sugar after overnight fasting of 10-14 hours. The elderly who were unable to come to the hospital were tested by using a glucometer (Optium Omega Meter manufactured by Abbott Diabetes Care Limited, Range Road Witney, Oxon Ox29, OYL UK).
A questionnaire was given to each member of the household who was ≥18 yr old. The elderly and children were explained the questions and their importance. The individuals were also interviewed about their family history of diabetes. This study protocol was approved by the Institutional Ethical Committee. The written informed consent was sought from all the participants before they were surveyed.
Questions were also asked to test their level of awareness regarding diabetes. The answers were recorded on a 5-pointer scale where 1 meant ‘Very Poor’ and 5 - ‘Excellent’. The overall care was calculated on the basis of their food habits, lifestyle, exercise and frequency of blood tests.
Data were analysed using Z test and Chi-square.
Results
In the study, 172 households (34.05%) had one or more known diabetes cases. The total number of subjects with diabetes in these households was 246 (11.29%) with a mean age of 60.21±10.91 yr and a mean duration of diabetes of 9.74±8.39 yr. There were 56 households which had more than one case of diabetes.
The condition was more common in males; 145 males were found to be diabetic that accounted for 58.94 per cent of all diabetic subjects. The remaining 41.06 per cent subjects with diabetes were females.
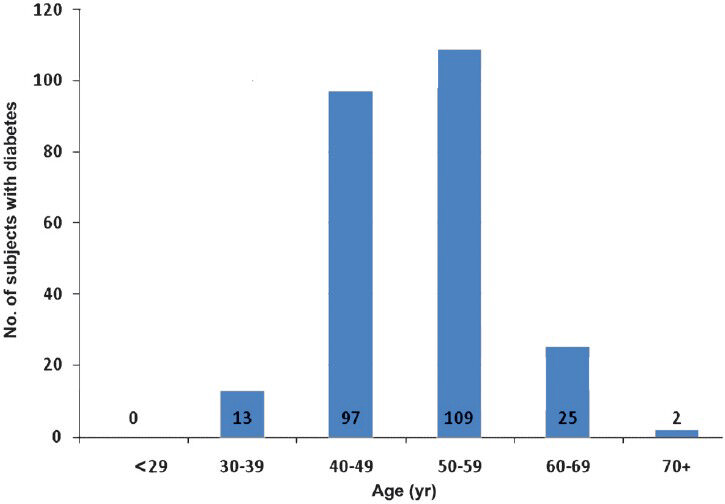
The highest occurrence of diabetes (22.01%) was found among the age group of 65-69 yr (Table). In 55.28 per cent cases, diabetes was first detected after the age of 50 years. All the 246 subjects developed diabetes after 25 yr of age. The age at diagnosis for majority (44.30%) of the diabetic subjects was during 50-59 yr. The average known age at onset of diabetes was found to be 50.46±7.27 yr. (Fig. 1).
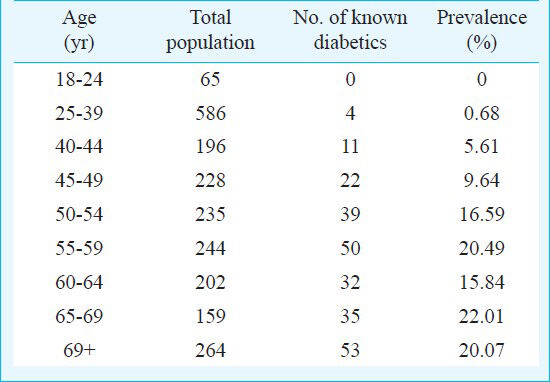
- Age group at which diabetes was first detected.
The number of relatives of index cases with diabetes are given in Figs 2 and 3. Among patients, 109 (44.30%) had at least one affected relative and 23 (9.34%) had at least two diabetic family members (P < 0.001).
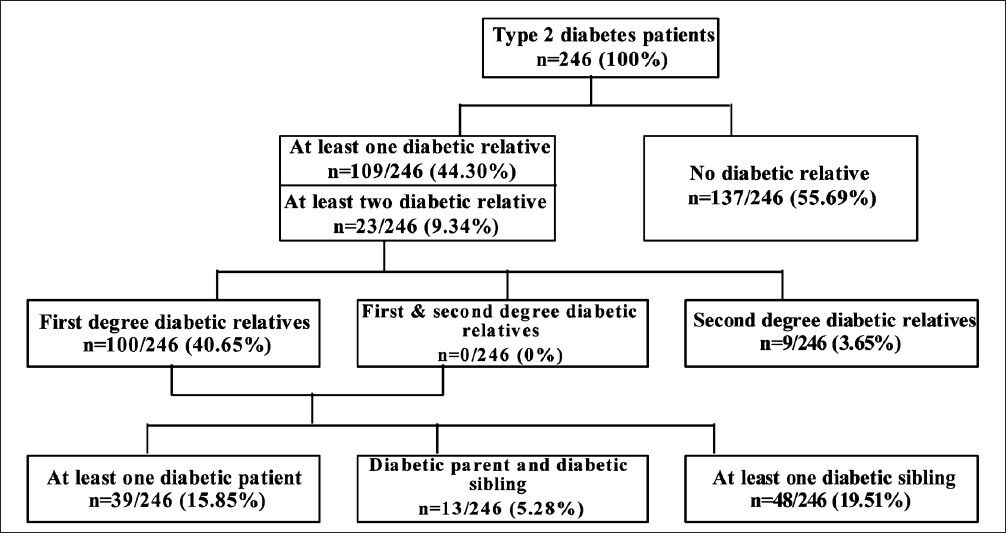
- Family history of diabetes in the studied population. Flow chart showing the frequency of diabetes in the relatives. Data are number (percentage in parenthesis) of index patients having at least one first or second degree relative with diabetes.
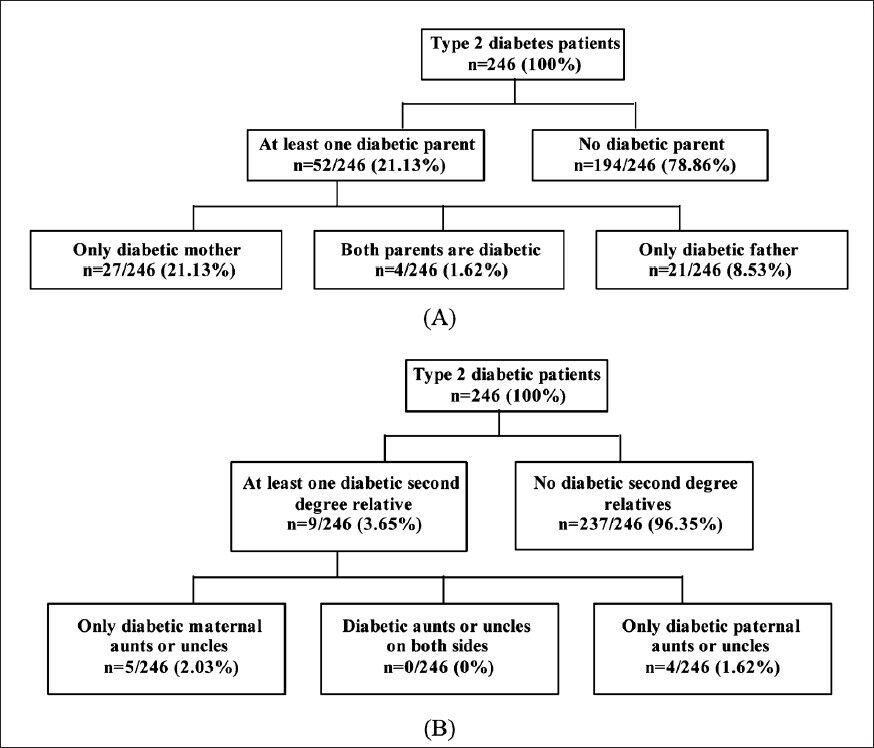
- Flow charts showing the frequency of diabetes in relatives. Data are number (percentage in parenthesis) of probands having (A) parents with diabetes and (B) second degree relatives with diabetes.
Since this is a very small and close knit community, in majority of the marriages the couples were related to each other. The Bohras are by and large non vegetarians. On the 5-pointer scale the average meal plan for diabetic subjects was found to be 3.78±0.52 while for non-diabetic subjects, it was 2.85±0.63 (P<0.001); 8.13 per cent diabetic subjects (n=20) were graded as ‘Excellent’ and 38.21 per cent (n=94) were graded ‘Poor’ on the 5 pointer scale regarding their daily exercise while the remaining were kept under the ‘Good’ category. The mean was found to be 2.67±0.66 (P < 0.01 compared to non diabetics). Similar observations were found in non-diabetic subjects (2.80±0.71) which showed that even after being diagnosed with diabetes, very few started to do exercise. More than 80 per cent men were businessmen and those employed were in jobs with desk work. A sedentary lifestyle could, therefore, be an important risk factor (2.76±0.60, P<0.001). The overall care for diabetes in diabetic subjects on the 5-pointer scale was 3.76±0.56 as compared to 2.86±0.60 in non-diabetic subjects (P<0.001).
The respondents were asked about their perception on the prevalence of diabetes in their community and the possible factors responsible for it. While most of the respondents were not aware about the prevalence of diabetes among them, and the factors that cause diabetes. Only 16 per cent of the non-diabetic subjects were found to have their blood tested for sugar as compared to 100 per cent of the diabetic subjects (P<0.001).
Discussion
The presence of diabetes in the ‘Dawoodi Bohra youth community’ was 11.29 per cent which was significantly higher than 3.8 per cent reported in India in general population1. The average age of onset of diabetes was 50.46±7.27 yr. This implies that these subjects developed diabetes in the most productive years of their life and both hereditary factors and lifestyle might have had a major role to play1. All the patients in our study had type 2 diabetes.
Maternal excess was also evident as 11 per cent of the diabetic subjects had a diabetic mother while 8.5 per cent had a diabetic father, which was in agreement with several other studies567812. The reason for this could be pregnancy, diabetic environment in utero, longer average life span or mitochondrial DNA mutations56812. Though this fact has been contradicted by certain other studies9 maternal transmission of type 2 diabetes remains debatable12.
Majority of the members led a sedentary life and all were non-vegetarians with a high intake of oil and fat in their meals. The present findings confirm to those of the past studies and exhibit a strong association between diabetes, socio-economic status, lifestyle habits, obesity and cardiovascular risk factors3.
Majority of the patients were diagnosed after the age of 50. The reason for this could have been low level of awareness among the people regarding their health. People generally avoided visiting doctors and consulted them only when the condition aggravated. Even after being diagnosed many of them did not take any measure to change their eating habits or perform physical exercise prescribed to them.
In conclusion, the present results showed that the marital alliances, familial aggregation and lifestyle be the key factors that enhanced the occurrence of diabetes in this community. This work also reflected poor awareness among the people of this community regarding their health related issues.
References
- Genetics, obesity and environmental risk factors associated with type 2 diabetes. Croat Med J. 2005;46:302-7.
- [Google Scholar]
- Diabetes: the cost of diabetes. Fall sheet No. 23r. Available from: http://www.who.int/mediacentre/factsheets/fs236/en
- [Google Scholar]
- Importance of family history in type 2 black South African diabetic patients. Postgrad Med J. 2001;77:323-5.
- [Google Scholar]
- Maternal effect and familial aggregation in NIDDM. The CODIAB study. CODIAB-INSERM-ZENECA Study Group. Diabetes. 1994;43:63-7.
- [Google Scholar]
- Diabetes in Hong Kong Chinese: Evidence for familial clustering and parental effects. Diabetes Care. 2000;23:1365-8.
- [Google Scholar]
- Familial aggregation and excess maternal transmission of type 2 diabetes in Tunisia. Postgrad Med J. 2007;83:348-51.
- [Google Scholar]
- Prevalence of diabetes mellitus amongst the Bhargavas in India. J Hum Ecol. 2005;17:137-41.
- [Google Scholar]
- Familial aggregation of type 2 (non-insulin dependent) diabetes mellitus in South India : absence of excess maternal transmission. Diabet Med. 1996;13:232-7.
- [Google Scholar]
- Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia. 2006. Report of a WHO/IDF Consultation. Available from: http://www.who.int/diabetes/publications/Definition%20and%20diagnosis%20of%20diabetes_new.pdf
- [Google Scholar]
- Determination of blood glucose using an oxidase - peroxidase system with a non - carcinogenic chromogen. J Clin Pathol. 1969;22:158-61.
- [Google Scholar]
- Familial history of type 2 diabetes in patients from Southern Brazil and its influence on the clinical characteristics of this disease. Arq Bras Endocrinol Metab. 2006;50:862-8.
- [Google Scholar]




