Translate this page into:
Predictors of atypical femoral fractures during long term bisphosphonate therapy: A case series & review of literature
Reprint requests: Dr Sanjay Bhadada, Associate Professor, Department of Endocrinology, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: bhadadask@rediffmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Bisphosphonates (BPs) are the most widely prescribed medicines for the treatment of osteoporosis because of their efficacy and favourable safety profile. There have been, several reports on an increased incidence of atypical femoral fractures after long term treatment with BPs. The objective of this study was to evaluate the clinical presentation including prodromal symptoms, skeletal radiograph findings, type and duration of BPs received and treatment outcome of patients who developed atypical femoral fractures during bisphosphonate therapy.
Methods:
In this retrospective study, eight patients with atypical femoral fractures were analysed based on clinical features, biochemical and radiological investigations.
Results:
Of the eight patients, who sustained atypical femoral fractures, six were on alendronate and two were on zoledronate therapy before the fractures. In addition to BPs, two patients were on long term corticosteroid therapy for rheumatoid arthritis and Addison's disease. Three patients had bilateral atypical femoral fractures. Except one, all of them had prodromal symptoms prior to fracture. Skeletal radiograph showed cortical thickening, pointed (beaking of) cortical margin and transverse fracture in meta-diaphyseal location. Serum calcium, phosphate, alkaline phosphatase (ALP) and intact parathyroid hormone (iPTH) concentrations were within the reference range in all patients.
Interpretation & conclusions:
Long term bisphosphonate therapy may increase the risk of atypical femoral fractures. Presence of prodromal pain, thickened cortex with cortical beaking may be an early clue for predicting the atypical fractures. High risk patients need periodical skeletal survey and a close follow up for early detection of cases.
Keywords
Atypical
bisphosphonates
femoral shaft
fracture
subtrochanteric

Bisphosphonates (BPs) are one of the most commonly used drugs in the prevention and treatment of osteoporosis1. These also used in the management of various other metabolic bone diseases like Paget's disease2, fibrous dysplasia3, osteogenesis imperfecta4 and bone metastasis5. Several randomized controlled trials with various BPs therapy have established their effectiveness in postmenopausal women by significantly increasing bone mineral density (BMD) and reducing the occurrence of osteoporotic fractures in hip as well as in spine.
BPs inhibit bone resorption by inducing apoptosis of osteoclasts6. Because of the prolonged skeletal half life of nitrogen containing BPs such as alendronate, risedronate and zoledronate, these might lead to oversuppression of bone turnover as well as bone formation, even after discontinuing the therapy7.
In 2005, Odvina et al8 published a case series of osteoporotic patients on long term bisphosphonate therapy who had acquired atypical femoral fractures. Bone histomorphometry revealed severely suppressed bone turnover (SSBT) with marked reduction in both bone formation and resorption9. Several other case series1011121314 have been published describing about the atypical femoral fractures. Reports linking long-term use of BPs with atypical fractures of the femur led the American Society for Bone and Mineral Research (ASBMR) to appoint a task force to address key questions related to this problem15.
We describe here eight cases of atypical femoral fractures developed during long term BPs therapy and their clinical presentation, radiological findings and treatment outcome.
Material & Methods
Non-comminuted, subtrochanteric fractures, located anywhere along the femur from just distal to the lesser trochanter to proximal to the supracondylar flare with transverse or short oblique orientation following minimal trauma (fall from a standing height or less) in subjects after long term BPs therapy were analyzed in the study. Long term BPs therapy was defined as more than one year use of either alendronate or two doses of zoledronate without any drug interval. The diagnosis of atypical femoral fractures was based on the “clear case definition” provided by the American Society for Bone and Mineral Research Task force15. The case definition includes major features and minor features.
This retrospective study was conducted between January 2010 and December 2012. Eight patients, all women, on long term alendronate (2-6 yr) once/week or zoledronate 3-8 doses therapy were available and included. Three patients were from Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, three from Command hospital, Chandigarh, and one from Medicity Medanta hospital, Gurgaon, and one from Rabindranath Tagore Medical College, Udaipur, India. All patients provided written informed consent for participation in the study. The permission from Institute ethics committee was taken to use data for research purpose.
Biochemical measurements: Laboratory studies were performed on the next day of visit in empty stomach. Serum samples were assayed for calcium, phosphate, alkaline phosphatase (ALP), intact parathyroid hormone (iPTH) and 25-hydroxyvitamin D [25(OH) vit D]. BMD of L2-L4 vertebrae, femoral neck and distal third of radius was measured by dual energy X-ray absorptiometry (Hologic QDR, MA,USA). It was done in different hospitals with different methods.
Results
Demographic features, indication and duration of bisphosphonate therapy, prodromal symptoms, location of fractures are summarized in the Table. The mean age of the patient was 60.4 yr (range 35 - 83 yr). Of the eight patients, six received alendronate and two zoledronate prior to fractures. The mean duration of bisphosphonate treatment received prior to fracture was 4.5 yr (range 2 - 6 yr). Two patients were on glucocorticoid therapy in addition to alendronate. Seven of the eight patients had dull aching pain at the site of fracture, before the actual fracture site. Serum calcium, phosphate, ALP and iPTH concentrations were within the reference range in all patients. Except one patient, all had serum 25(OH) Vit D levels > 30 ng/ml.
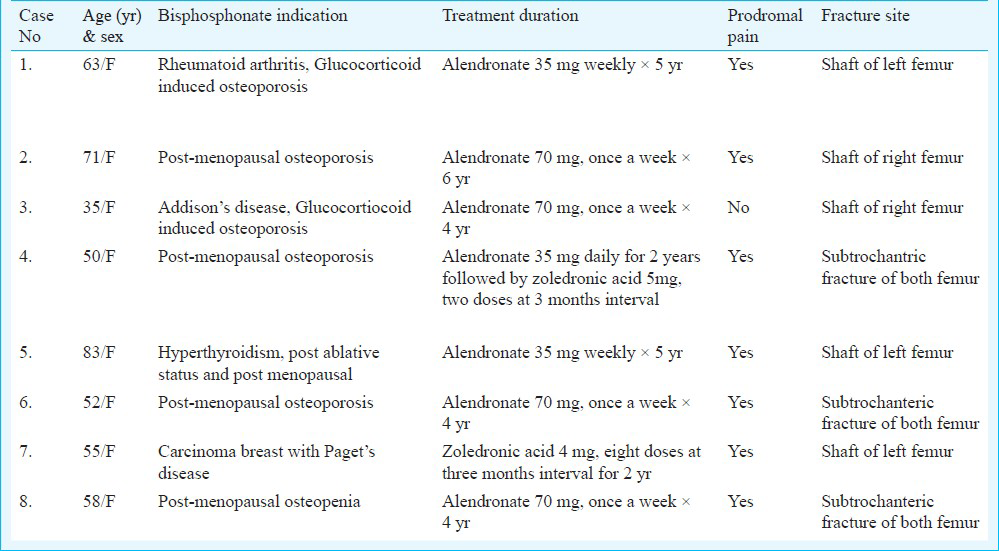
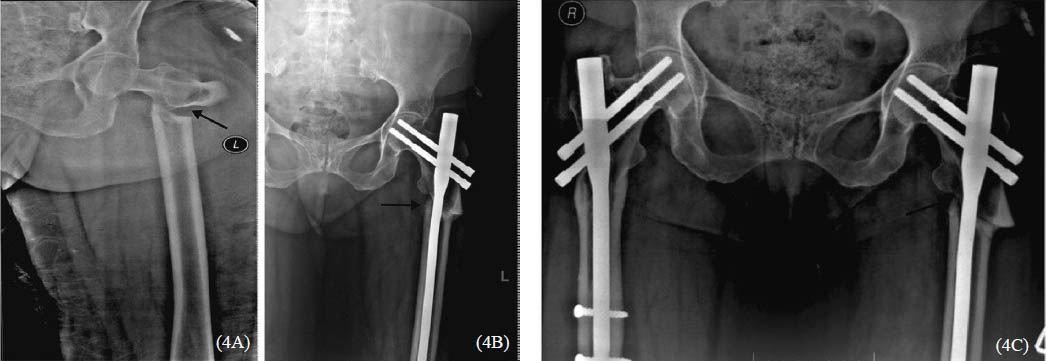
Individual X rays are shown Figs 1 to 8) to highlight the unusual location and type of fractures as well as presence of relatively thick cortices. Patient number 4, 6 and 8 had bilateral fractures (Figs. 4,6,8) which required intra-medullary nailings. The major radiological features noted were cortical thickening in the lateral side of subtrochanteric region, medial cortical spike (cortical beaking, Figs. 1A, 2A) and short oblique (Fig. 3A) and/ or transverse fractures (Figs. 4,5). BMD showed osteoporosis in two patients (patients no 4 and 5) and low bone density (osteopenia) in the remaining six patients. Due to the delayed healing all except one underwent orthopaedic surgical procedures in the form of intramedullary nailing with fixation.
- Radiograph of a 63 yr old woman showing cortical beaking at the site of prodromal pain (arrow), followed by fracture and intramedullary nailing for fracture left shaft of femur.
-
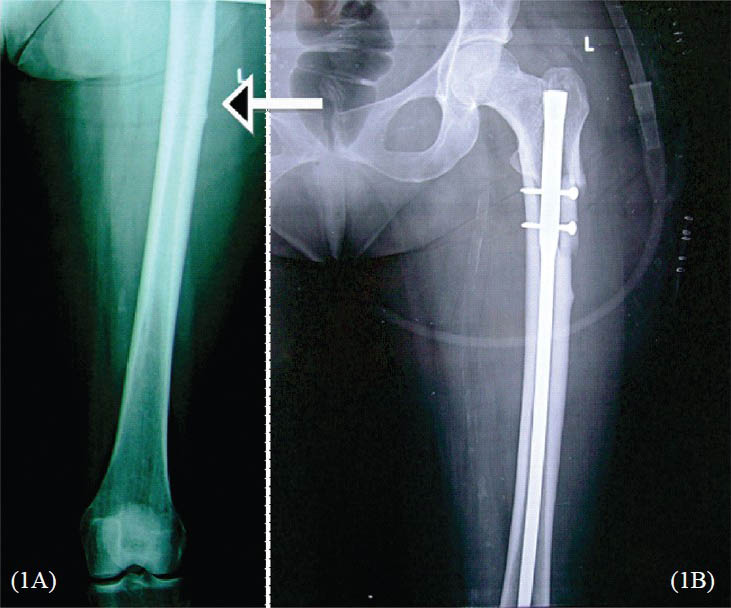
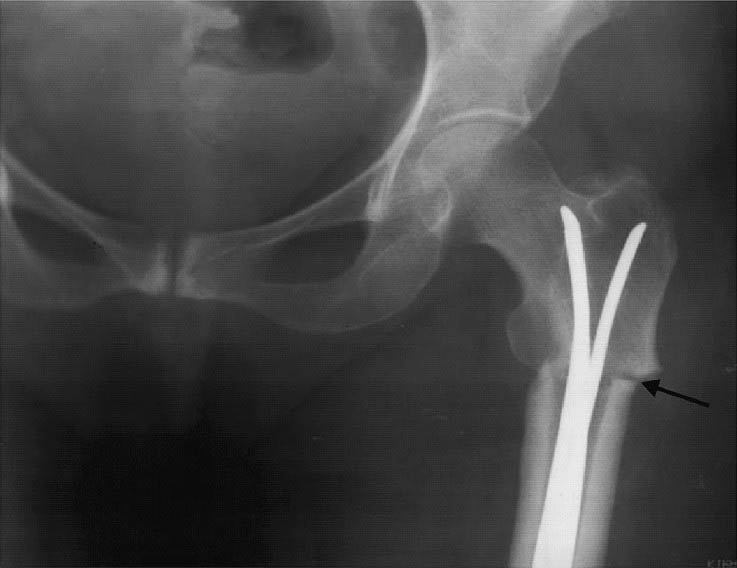
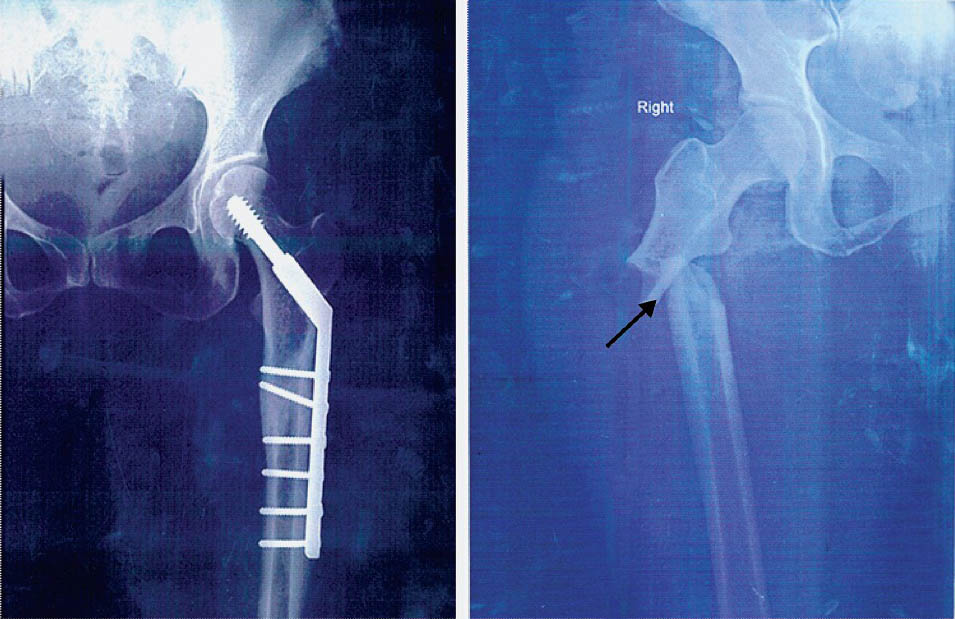
A. Radiograph of a 71 yr old woman showing cortical beaking findings in the shaft right femur (arrow). 2B. Bone scan showing small hot spot in the right proximal femur correlating with the site of stress fracture.
-
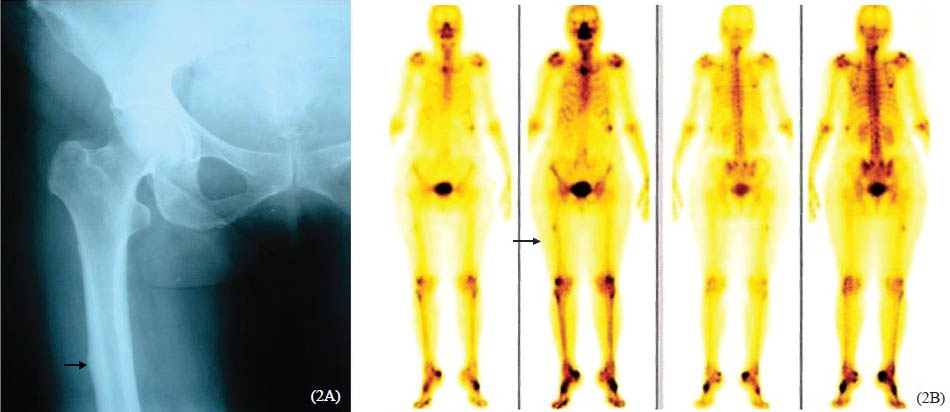
A. Radiograph of a 35 yr old woman showing subtrochanteric fracture of right femur (arrow). 3B. Radiograph showing callus formation with intramedullary nailing in right shaft of femur.
-
A. X-ray pelvis AP view showing subtrochanteric fracture of shaft of left femur. 4B. X-ray pelvis AP view showing subtrochanteric fracture of shaft of left femur with nailing. 4C. X-ray pelvis AP view showing bilateral subtrochanteric fracture of shaft of femur with nailing.
- Radiograph an 83 yr old woman showing thick cortices with subtrochanteric fracture and intramedullary nail.
-
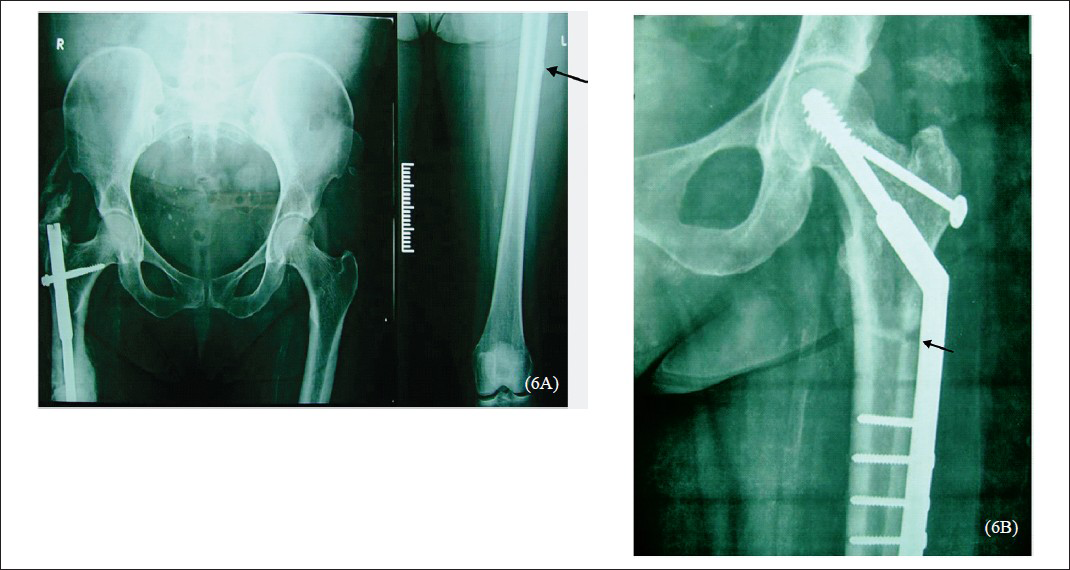
A. Radiograph a 52 yr old woman showing subtrochanteric fracture of right femur with intramedullary nail and cortical beaking of left femur (arrow). 6B. Radiograph showing subtrochanteric femur of left femur with external fixation showing thickened cortices and fracture union (arrow).
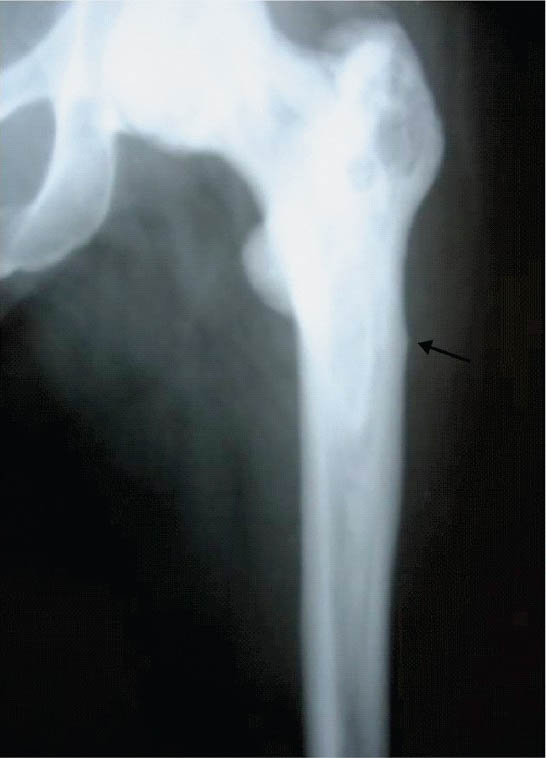
- Radiograph of a 55 yr old woman showing the cortical beaking (arrow) of left femur in patients with Paget's disease and greater trochanter showing the lytic and sclerotic lesions.
- Radiograph of a 58 yr old woman of pelvis AP view nailing showing the left subtrochanteric fracture with followed by right subtrochanteric fracture (arrow).
Case 1 was a 63 yr old, post-menopausal female with steroid dependent rheumatoid arthritis who received alendronate 35mg once weekly for five years along with calcium and vitamin D. Her BMD by DXA scan showed T-scores of -1.2, -0.1 and Z scores of -0.1 and 0.4 at lumbar spine and hip, respectively. She presented with fracture of shaft of her left femur following a trivial trauma (Fig. 1A). Preceding the injury, she complained of pain in her left thigh while walking. Her medications included prednisolone (10mg/day), hydroxychloroquine and leflunamide. Investigation revealed albumin adjusted serum calcium 8.8 mg/dl, phosphorus 4.7 mg/dl, alkaline phosphatase 134 (60-120 U/l), intact PTH 17.9 pg/ml (10-65) and 25 hydroxy vitamin D 14.4 ng/ml. Radiographs revealed a horizontal fracture in the proximal shaft of left femur with small stress fracture on the corresponding site on the right femur with apparently normal bone density. Following the fracture alendronate was discontinued and treated with inj Teriparatide 20 μg subcutaneous (SC) daily for one year (Fig. 1B).
Case 2 was a 71 yr old post-menopausal female on treatment with oral alendronate 70mg/week along with daily calcium and vitamin D for 6 yr who developed pain in the upper part of her right thigh of one month duration. Before bisphosphonate treatment her BMD T score in spine and femoral neck was -1.6 and -1.1, respectively. There was no history of trauma, or past history of fractures, steroid use, smoking or alcohol use. X-ray (Fig. 2A) showed a stress fracture in the upper shaft of right femur. Bone scan (Fig. 2B) showed a hot spot in the same region. Calcium profile, iPTH and 25 (OH) vit D levels were within normal range. She has been advised to stop alendronate and to continue calcium and vitamin D and precautions to avoid fall and to repeat BMD after one yr.
The third case was of a 35 yr old pre-menopausal female with Addison's disease on treatment with prednisolone for 5 years. She received alendronate 70mg/week with calcium and vitamin D for osteopenia for the past four years. Before bisphosphonate treatment her BMD T scores were -2.1 at the spine and -1.75 at the femoral neck and Z score of -2.0 and 1.7, respectively. Her albumin adjusted serum calcium was 9.8 mg/dl, phosphorus 4.1 mg/dl, alkaline phosphatase 98 (60-120 U/l), intact PTH 25 pg/ml (10-65) and 25 hydroxy vitamin D 75.9 ng/ml. She sustained a fracture of shaft of right femur after a fall from standing height (Fig. 3A). Because of delayed healing with poor callus formation she underwent intramedullary nailing (Fig. 3B).
The fourth case was of a 50 yr old post-menopausal female with osteoporosis and past history of fracture neck of right femur. She was treated with alendronate 35 mg daily for two years followed by zoledronic acid 5mg, two doses at three months interval, along with calcium and vitamin D. She developed pain in the left thigh, and after a few months developed a spontaneous subtrochanteric fracture of left shaft of femur (Fig. 4A) without any fall. Her biochemical investigation revealed albumin adjusted serum calcium of 9.4 mg/dl, iPTH 18pg/ml, 25 (OH) vit D 34.4 ng/ml, procollagen 1 amino-peptide (P1NP) 20.2ng/ml (Reference range, RR 16-73), osteocalcin 2.0ng/ml (RR 3.1-13.7) and bone specific ALP 17.3 u/l (RR 14.2 - 42.7). Her BMD T scores at left forearm and spine were -1.24 and -2.74, respectively. This patient also underwent intramedullary nailing because of delayed healing (Fig. 4B). Fig. 4C shows the bilateral fracture of femur.
Case 5 was of an 83 yr old post-menopausal female with post ablative hypothyroidism who was treated with alendronate 35mg once weekly along with calcium and vitamin D for five years for osteoporosis. Her BMD by DXA scan showed T-scores of -2.8, -2.3 at lumbar spine and hip, respectively. She had pain in her left thigh for a period of two months followed by a fracture of left femoral shaft without any fall (Fig. 5).
The sixth case was a 52 yr old post-menopausal female with known type 2 diabetes mellitus, who was diagnosed as osteoporosis and treated with alendronate 70mg/week, calcium and vitamin D for the past four years. Her baseline BMD was not available. She sustained a fracture of right sub-trochanteric femur following a fall from standing height (Fig. 6A). Her left femur X-ray also showed cortical beaking. Her BMD T scores at the time of fracture were -1.1 at femoral neck and -0.3 at lumbar spine. Her albumin adjusted serum calcium was 8.9 mg/dl, phosphorus 4.6 mg/dl, alkaline phosphatase 82 (60-120 U/l), intact PTH 56 pg/ml (RR, 10-65) and 25 hydroxy vitamin D 32 ng/ml. She was subjected to intra-medullary nailing of right femur due to poor healing. Six months later, after the index fracture, this patient sustained a new fracture in the opposite femur following a trivial trauma (Fig. 6B).
The seventh case was of a 55 yr old female with known case of carcinoma right breast and Paget's disease, who received eight doses of zoledronic acid (4 mg) at three monthly intervals for prevention of bony metastasis and treatment of Paget's disease over two years. Her baseline BMD T scores were -1.4 at femoral neck and -1.1 at lumbar spine. Her periodic skeletal survey of Paget's disease showed thickened cortices with pointed cortical margin (Fig. 7) in its lateral border. Her procollagen 1 amino-peptide (P1NP) level was 32 ng/ml (RR 16-73). Zoledronic acid was stopped and treated with calcium and vitamin D for past three months.
The last case was a 58 yr old female with post surgical menopause for the past 14 yr. She sustained a subtrochanteric fracture of left femur without any fall. She had a diffuse dull aching pain over the left thigh for a period of three months prior to fracture. She received alendronate 70mg/week with calcium and vitamin D for the past four years. Her BMD T scores at the time of fracture were -0.6 at right femoral neck and -0.8 at lumbar spine. Her albumin adjusted serum calcium was 9.8 mg/dl, phosphorus 4.7 mg/dl, iPTH 33.5 pg/ml and 25(OH) D 32 ng/ml. She underwent external fixation for the left subtrochanteric fracture (Fig. 8A). Two years after the first fracture, she sustained a trivial fall in wash room. Her X-ray revealed right subtrochanteric fracture with thickened cortices (Fig. 8B). She was treated with open reduction and internal fixation of right femur.
All patients were followed up for the mean duration of 1.2 yr (range 3 - 0.6 yr) after the occurrence of the first fracture. Due to the delayed healing, (non union and poor callus formation after three months of immobilization), five patients underwent orthopaedic surgical procedures in the form of intra-medullary nailing with fixation. BPs were stopped; calcium and vitamin D were continued in all the patients of atypical femoral fractures in the present study.
Discussion
In our patients, all fractures occurred during normal daily activities without any trauma or fall. Except one, all had prodromal symptom in the form of dull aching pain in the region of their atraumatic fractures. This prodromal pain is one of the classical features noted in our patients. An unusual feature noted in the radiographs that was common to all patients was cortical thickening. It was seen regardless of the age of the patient, underlying rheumatoid arthritis, Paget's disease or steroid therapy. Four of our patient had pointed cortical margin, early sign of impending fracture. On follow up, the patients had fracture at the same site indicating that thickening of cortices might indeed be the initial clue to the impending shaft fractures especially if associated with prodromal pain.
From the literature review, majority of fracture occurred after oral alendronate therapy (>95%) and remaining were with oral risedronate, intravenous pamidronate and zoledronate15. The duration of bisphosphonate therapy ranged from 1.3 to 17 yr, with median duration of 7 yr. Very few reports included bone turnover markers (BTM), and only a minority of cases BTM had been suppressed910.
BPs accumulate in the hydroxyapatite mineral phase of long bone and enter into osteoclasts, reduce resorption through inhibition of farnesyl pyrophosphate synthase (FPPS), an enzyme in the mevolonate to cholesterol pathway. Inhibition of FPPS interferes with isoprenylation of small guanosine triphosphatases (GTPases) in the osteoclasts and disrupts the attachement of osteoclasts to the bone surface, which inhibits resorption and inducing osteoclast apoptosis916.
Bisphosphonate therapy, by suppressing the bone turnover impairs the bone's ability to repair strain related microdamage and leads to accumulation of microcracks with compromised bone strength1017. Use of additional antiresorptive therapies (estrogen, calcitonin or raloxifene), presence of rheumatoid arthritis, chronic glucocorticoid therapy and presence of prodromal pain in the thigh or groin are high risk factors for future development of bisphosphonate fractures, and need to be monitored closely. Recently proton pump inhibitors (PPI) usage was shown to be associated with increased fracture incidence1819. However, none of our patient had chronic use of PPI or H2 blocker therapy.
Reports of osteonecrosis of jaw20 and atypical femoral fractures101112131421222324252627 have led to suspect about skeletal safety of long term bisphosphonate therapy. The optimal duration of bisphosphonate therapy for post-menopausal osteoporosis and all other conditions for which BPs are used, remains unclear. Because bisphosphonates are avidly bound to bone, a reservoir of drug accumulates after years of treatment that is gradually released over months or years. This makes it possible to consider drug holidays for 3-5 yr (time off bisphosphonate therapy) and then resuming therapy. Many of our patients received BPs even with normal BMD indicating overuse of the bisphosphonates.
Though, the association between atypical femoral fractures and bisphosphonate use has been noted in the present study as well as in many earlier studies101112131421222324252627, there are some reports which negate this association. The increasing prevalence of atypical femoral fracture following bisphosphonate use is only an association and for a clear causal link, long term prospective studies are needed. The risk–benefit ratio still remains favourable for the use of bisphosphonates to prevent fractures.
The presence of prodromal pain and radiograph evidence of cortical beaking with thick cortices are potential signs to predict atypical femoral fractures. BPs need to be stopped in such patients and bone formation and suppression markers to be assessed. Ensuring adequate calcium and vitamin D intake both before initiation and after stopping BPs therapy is extremely important. Since BPs inhibit osteoclastic remodelling, endochondral fracture repair is the preferred method of surgical treatment in complete atypical femoral fracture patients15. Intramedullary reconstruction full-length nails accomplish this goal and protect the entire femur. Recombinant human parathyroid hormone (rhPTH) is a promising osteoanabolic agent with potential therapeutic benefit, which increases the number and function of osteoblast as well as accelerates the fracture healing.
BPs are still widely used drugs for osteoporosis. Although there are concerns regarding the atypical femoral fractures, the overall incidence of these atypical fractures is still very rare compared to the number of typical osteoporotic fractures prevented. The decision to initiate treatment with a bisphosphonate, and how long to treat, should be based on thoughtful assessment of the balance between the expected benefit and potential risks.
In conclusion, Long term bisphosphonate therapy may increase the risk of atypical femoral fractures. Presence of prodromal pain, thickened cortex and/ or cortical beaking may be an early clue for predicting the atypical fractures. The informed and judicious use of bisphosphonates confers a clear clinical benefit in most carefully selected patients that outweighs potential risks associated with its use.
References
- Comparison of a single infusion of zoledronic acid with risedronate for Paget's disease. N Engl J Med. 2005;353:898-908.
- [Google Scholar]
- Medical therapy in adults with fibrous dysplasia of bone. J Bone Miner Res. 2006;21(Suppl 2):114-7.
- [Google Scholar]
- Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med. 1998;339:947-52.
- [Google Scholar]
- Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial. Cancer J. 2001;7:377-87.
- [Google Scholar]
- Mechanisms of action of bisphosphonates: similarities and differences and their potential influence on clinical efficacy. Osteoporos Int. 2008;19:733-59.
- [Google Scholar]
- Effects of suppressed bone turnover by bisphosphonates on microdamage accumulation and biomechanical properties in clinically relevant skeletal sites in beagles. Bone. 2001;28:524-31.
- [Google Scholar]
- Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005;90:1294-301.
- [Google Scholar]
- Unusual mid-shaft fractures during long-term bisphosphonate therapy. Clin Endocrin (Oxf). 2010;72:161-8.
- [Google Scholar]
- Severely suppressed bone turnover and atypical skeletal fragility. J Clin Endocrinol Metab. 2008;93:2948-52.
- [Google Scholar]
- Subtrochanteric stress fractures in six patients on long term bisphosphonate therapy: a case series. Bone. 2009;44:S77-78.
- [Google Scholar]
- Bisphosphonate use and atypical fractures of the femoral shaft. N Engl J Med. 2011;364:1728-37.
- [Google Scholar]
- Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res. 2012;27:2544-50.
- [Google Scholar]
- American Society for Bone and Mineral Research Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010;25:2267-94.
- [Google Scholar]
- Further insight into mechanism of action of clodronate: inhibition of mitochondrial ADP/ATP translocase by a nonhydrolyzable adenine-containing metabolite. Mol Pharmacol. 2002;61:1255-62.
- [Google Scholar]
- Bisphosphonate treatment suppresses not only stochastic remodeling but also the targeted repair of microdamage. Calcif Tissue Int. 2001;69:281-6.
- [Google Scholar]
- The effect of proton pump inhibitors on fracture risk: report from the Canadian Multicenter Osteoporosis Study. Osteoporos Int. 2013;24:1161-8.
- [Google Scholar]
- Use of proton pump inhibitors and risk of hip fracture in relation to dietary and lifestyle factors: a prospective cohort study. BMJ. 2012;344:e372.
- [Google Scholar]
- Osteonecrosis of jaw associated with bisphosphonate use. Indian J Endocrinol Metab. 2012;16:450-2.
- [Google Scholar]
- Subtrochanteric insufficiency fractures in patients on alendronate therapy: a caution. J Bone Joint Surg Br. 2007;89:349-53.
- [Google Scholar]
- An emerging pattern of subtrochanteric stress fractures: a long-term complication of alendronate therapy? Injury. 2008;39:224-31.
- [Google Scholar]
- Low-energy femoral shaft fractures associated with alendronate use. J Orthop Trauma. 2008;22:346-50.
- [Google Scholar]
- Bone turnover in bone biopsies of patients with low-energy cortical fractures receiving bisphosphonates: a case series. Calcif Tissue Int. 2009;85:37-44.
- [Google Scholar]
- Low-energy femoral fractures associated with the long-term use of bisphosphonates: a case series from a Swiss university hospital. Drug Safety. 2009;32:775-85.
- [Google Scholar]
- Bilateral low-energy simultaneous or sequential femoral fractures in patients on long-term alendronate therapy. J Bone Joint Surg Am. 2009;91:2556-61.
- [Google Scholar]
- Atypical femoral fractures and bisphosphonate treatment: experience in two large United Kingdom teaching hospitals. J Bone Joint Surg Br. 2012;94:385-90.
- [Google Scholar]




