Translate this page into:
Relationship of household air pollution from solid fuel combustion with tuberculosis?
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Household air pollution (HAP) from combustion of solid biomass fuel (such as dried-dung, wood and crop residue) for cooking and heating purposes, has emerged as an important risk factor in the pathogenesis, prevalence, morbidity and mortality from chronic respiratory diseases such as chronic bronchitis (CB), chronic obstructive pulmonary disease (COPD) and asthma12345. Exposure to HAP also accounts for frequent occurrence of respiratory infections and lung function impairment particularly in children678. There are inconsistent data on association of HAP with respiratory infections in adults. In the recent past, there have been reports on the role of HAP as a risk factor for tuberculosis (TB)910. But the evidence has been sparse, and mostly from the small studies.
It is known that TB occurs more often among inmates of slums with poor living conditions111213. The poor living conditions include the environmental pollution from use of solid fuels for combustion for cooking and heating, widely prevalent in these areas. A systematic review of 33 studies on tobacco smoke, indoor air pollution and TB in 2007, including five on biomass fuel combustion concluded that the exposures increased the risk of TB, but stronger evidence was needed before the final conclusions could be drawn14.
Of the 994 full text articles, only 10 possible articles were found by the authors searching for an association of indoor fuel combustion (IAP) and TB15. Only three of the six studies which met the inclusion criteria for the systematic review reported a significant risk of TB amongst the exposed subjects15. In another meta-analysis in 2012, an extensive review of literature revealed 10 studies which showed a pooled odds ratio (OR) of 1.55 (95% C.I. 1.11 - 2.18) for TB in indoor air pollution (IAP) exposed individuals16. There were eight case control studies of which three did not show any significant association16171819. On the other hand, both the cross-sectional studies from India as well as five case control studies from India, Benin, Mexico and Nepal, respectively showed significant risk of exposure1620212223242526. Some of the studies had classified variable odds ratio with different types of fuels used in the kitchen or with reference to present and past exposure2526. No association was shown in a recent report on 355 TB cases from Directly Observed Therapy Centres and 804 controls from the neighbourhoods of patients from rural settings of Sidama zone in South Ethiopia27. The study, however, suffered because of the low statistical power as pointed out by the authors themselves. The neighbourhood controls which they selected were over-matched and inappropriate to measure this ‘slight’ association in the presence of similarities of non-risk factor exposures27.
Most of the studies available on the subject are small in size based on a case-control design. Such a design is subject to variations depending upon the methods used to assess the exposure. This was evident by the presence of significant heterogeneity in different studies. None of these studies had employed any objective parameter of pollutant exposure. Some of the studies report an attempt at sub-categorization of exposure. The Benin study reported a higher risk (OR > 1) for use of solid-fuels for cooking on univariate analysis24. On multivariate analysis using other significant variables as well, the association was no longer significant24. Similarly, in a Delhi study, the TB risk was significantly influenced by the location of the kitchen and the presence of respiratory symptoms while cooking, but the TB odds did not significantly differ with the type of fuel used for cooking28. An earlier study from India reported a high OR of 3.26 (95% CI 1.25 – 8.46) for TB with “not having a separate kitchen” while the authors had also reported no significant association with the use of biomass fuels18. Such observations only point to the difficulties of exposure assessment. It is not uncommon in India and many other developing countries to have a working indoor kitchen to cook food within the one or two room living dwellings or huts. It is presumable that the environment of such dwellings gets highly polluted from combustion of solid (biomass) fuels.
There are several limitations to conduct large epidemiological studies because of the numbers of variables and other confounders which play an important role in causing TB. History of tobacco smoking, consumption of alcohol and presence of co-morbidities such as diabetes and human immunodeficiency virus (HIV) infection are some of the important risk factors for TB2930. The chances of infection with mycobacteria are also high among contacts of TB patients living closely in crowded homes with poor ventilation. Overcrowding, urbanization and industrialization in highly populated cities and towns are also responsible for an increased incidence of TB3132.
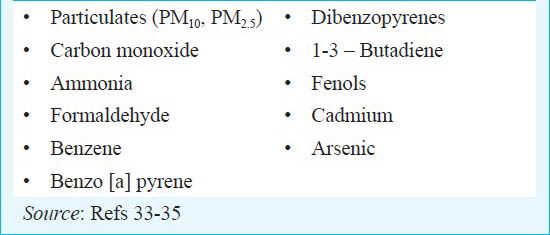
There are a large number of constituents of smoke emanating from combustion of solid, biomass fuels which are similar to those of tobacco smoke. A partial list of some toxic pollutants of tobacco smoke selected from the Federal Register, which are common to those of solid fuels taken from other sources is provided333435. This points to the obvious possibility of common toxicities such as carcinogenesis, increased allergic sensitization and reduced pulmonary defenses. Besides these constituents, there are several other noxious constituents of solid fuels such as gaseous products (ozone, nitric oxide, nitrogen dioxide, carbon dioxide, sulphur oxides) and metals (lead, manganese, selenium, calcium, mercury, silicon) which are likely to produce damage to the respiratory tract and impair mucociliary defenses3435.
The concentrations of the pollutants in the indoor air are particularly high as has been shown in numerous studies from several developing countries343536. The duration of exposure to the indoor air is prolonged and persistent. These factors make the lungs continuously exposed to inhaled air, as more vulnerable to the harmful effects of pollutants, such as the lower respiratory tract infections, including tuberculosis. There are experimental data which show the impairment of immune defenses on exposure to wood smoke. Inhalation of wood smoke in rabbits caused impairment of macrophage function, impaired mucociliary function and reduced bacterial clearance373839. All these functions are known to increase the chances of TB infection.
There are no studies on the effects of exposure to biomass fuel combustion on clinical features and mortality from tuberculosis. Similarly, influence of exposure on treatment effects and outcomes are not known. Assumptions can however, be made based on the known harmful effects of the combustion-smoke on the respiratory symptoms. Exposure to biomass combustion smoke is independently responsible for the presence of increased respiratory symptoms, chronic bronchitis and asthma454041. TB patients, therefore, in the presence of continued exposure to indoor combustion of biomass fuels are likely to suffer from exaggerated and prolonged symptoms and disease complications. Tobacco smokers with TB are more likely to suffer from chronic cough and sputum smear positive tuberculosis42. Tobacco smoking has been comincingly shown to relate to TB mortality4344454647. If one takes the smoking analogy, it can be presumed that the outcomes are likely to be poorer and mortality higher in the IAP exposed patients.
In conclusion, the indoor exposure to biomass fuel combustion used for heating and cooking is an identifiable risk factor for TB with demonstrable higher odds ratios in most studies. This is a subject which needs further investigations to clearly define the disease association, morbidity and mortality. Because of the potential implications as a treatment modifying factor and on outcomes of therapy, the issue has also got an important role in TB control programmes from public health point of view.
References
- Household air pollution is a major avoidable risk factor for cardio-respiratory disease. Chest. 2012;142:1308-15.
- [Google Scholar]
- Indoor air pollution in developing countries: a major environmental and public health challenge. Bull World Health Organ. 2000;78:1078-92.
- [Google Scholar]
- Biomass fuels, air pollution and health. In: A global review. New York: Plenum Press; 1987.
- [Google Scholar]
- Indian study on epidemiology of asthma, respiratory symptoms and chronic bronchitis in adults (INSEARCH) Int J Tuberc Lung Dis. 2012;16:1270-7.
- [Google Scholar]
- The effect of biomass fuel exposure on the prevalence of asthma in adults in India – review of current evidence. J Asthma. 2014;51:136-41.
- [Google Scholar]
- Indoor air pollution from unprocessed solid fuel use and pneumonia risk in children aged under five years: a systematic review and meta-analysis. Bull World Health Organ. 2008;86:390-8.
- [Google Scholar]
- Respiratory disease associated with solid biomass fuel exposure in rural women and children systematic review and meta-analysis. Thorax. 2011;66:232-9.
- [Google Scholar]
- Respiratory abnormalities and ventilatory capacity in a Papua New Guinea island community. Am Rev Respir Dis. 1976;114:537-48.
- [Google Scholar]
- Indoor fuel exposure and the lung in both developing and developed countries: an update. Clin Chest Med. 2012;33:649-65.
- [Google Scholar]
- Tobacco and tuberculosis: a qualitative systematic review and meta-analysis. Int J Tuberc Lung Dis. 2007;11:1049-61.
- [Google Scholar]
- Role of socio-economic factors in tuberculosis prevalence. Indian J Tuberc. 2004;51:27-31.
- [Google Scholar]
- Socio-economic differentials in mortality risk among men screened for the multiple risk factor intervention trial: I. White men. Am J Public Health. 1996;86:486-96.
- [Google Scholar]
- The increasing disparity in mortality between socio-economic groups in the United States. 1960 and 1986. N Engl J Med. 1993;329:103-9.
- [Google Scholar]
- Tobacco smoke, indoor air pollution and tuberculosis: a systematic review and meta-analysis. PLoS Med. 2007;4:e20.
- [Google Scholar]
- Indoor solid fuel combustion and tuberculosis: is there an association? Int J Tuberc Lung Dis. 2010;14:6-14.
- [Google Scholar]
- Indoor air pollution and the lung in low-and medium-income countries. Eur Respir J. 2012;40:239-54.
- [Google Scholar]
- Indoor solid fuel use and tuberculosis in China: a matched case-control study. BMC Public Health. 2011;11:498.
- [Google Scholar]
- An epidemiological evaluation of risk factors for tuberculosis in South India: a matched case control study. Int J Tuberc Lung Dis. 2006;10:80-6.
- [Google Scholar]
- Tuberculosis and gender: exploring the patterns in a case control study in Malawi. Int J Tuberc Lung Dis. 2004;8:194-203.
- [Google Scholar]
- Cooking with biomass fuels increases the risk of tuberculosis. Natl Fam Health Surv Bull. 1999;13:1-4.
- [Google Scholar]
- A study of household environmental risk factors pertaining to respiratory diseases. Energy Environ Monitor. 1997;13:61-7.
- [Google Scholar]
- Biomass fuel and risk of tuberculosis: a case-control study from Northern India. J Epidemiol Community Health. 2012;66:457-61.
- [Google Scholar]
- Association between biomass fuel and pulmonary tuberculosis: a nested case-control study. Thorax. 2009;64:705-8.
- [Google Scholar]
- Exposure to combustion of solid fuel and tuberculosis: a matched case-control study. Eur Respir J. 2011;38:132-8.
- [Google Scholar]
- Indoor pollution as an occupational risk factor for tuberculosis among women: a population-based, gender oriented, case-control study in Southern Mexico. Rev Invest Clin. 2009;61:392-8.
- [Google Scholar]
- Tuberculosis and indoor biomass and kerosene use in Nepal: a case-control study. Environ Health Perspect. 2010;118:558-64.
- [Google Scholar]
- Use of biomass fuel in households is not a risk factor for pulmonary tuberculosis in South Ethiopia. Int J Tuberc Lung Dis. 2014;18:67-72.
- [Google Scholar]
- Domestic cooking fuel exposure and tuberculosis in Indian women. Indian J Chest Dis Allied Sci. 2010;52:139-43.
- [Google Scholar]
- Risk of tuberculosis from exposure to tobacco smoke: a systemic review and meta analysis. Arch Intern Med. 2007;167:335-42.
- [Google Scholar]
- Tuberculosis and human immunodeficiency virus infection: recommendations of the Advisory Committee for the Elimination of Tuberculosis (ACET) MMWR Morb Mortal Wkly Rep. 1989;38:236-8.
- [Google Scholar]
- Resurgent tuberculosis in New York City. Human immunodeficiency virus, homelessness, and the decline of tuberculosis control programmes. Am Rev Respir Dis. 1991;144:745-9.
- [Google Scholar]
- Endemic tuberculosis among homeless men in New York City. Arch Intern Med. 1994;154:2069-73.
- [Google Scholar]
- Department of Health & Human Services; Food and Drug Administration. Harmful and potentially harmful constituents in tobacco products and tobacco smoke; Established list. Federal Register. 2012. 77 Available from: www.federalregister.gov
- [Google Scholar]
- Indoor air quality. In: Air quality guidelines – Global update. Vol 205. Denmark: WHO Regional Office for Europe; 2005. p. :189-216.
- [Google Scholar]
- Kerosene: a review of household uses and their hazards in low and middle income countries. J Toxicol Environ Health B Crit Rev. 2012;15:396-32.
- [Google Scholar]
- Rabbit lung after acute smoke inhalation. Cellular responses and scanning electron microscopy. Arch Surg. 1984;119:956-9.
- [Google Scholar]
- Regulation of mucociliary clearance in health and disease. Eur Respir J. 1999;13:1177-88.
- [Google Scholar]
- Alterations in the antibacterial properties of rabbit pulmonary macrophages exposed to wood smoke. Am Rev Respir Dis. 1984;129:76-81.
- [Google Scholar]
- Forum of International Respiratory Studies (FIRS) Task Force on Health Effects of Biomass Exposure. Biomass fuels and respiratory diseases: a review of the evidence. Proc Am Thorac Soc. 2008;15:577-90.
- [Google Scholar]
- Respiratory symptoms in Indian women using domestic cooking fuels. Chest. 1991;100:385-8.
- [Google Scholar]
- Smoking and pulmonary tuberculosis, an analysis based on a study of volunteers for mass miniature radiography. Tubercle. 1967;48:219-26.
- [Google Scholar]
- Smoking and mortality from tuberculosis and other diseases in India: retrospective study of 43000 adult male deaths and 35000 controls. Lancet. 2003;362:507-15.
- [Google Scholar]
- Emerging tobacco hazards in China: 1. Retrospective proportional mortality study of one million deaths. BMJ. 1998;317:1411-22.
- [Google Scholar]
- Tobacco associated mortality in Mumbai (Bombay) India. Results of the Bombay Cohort Study. Int J Epidemiol. 2005;34:1395-402.
- [Google Scholar]




