Translate this page into:
A rare cause of left back pain
*For correspondence: Chu5583@ms55.hinet.net
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
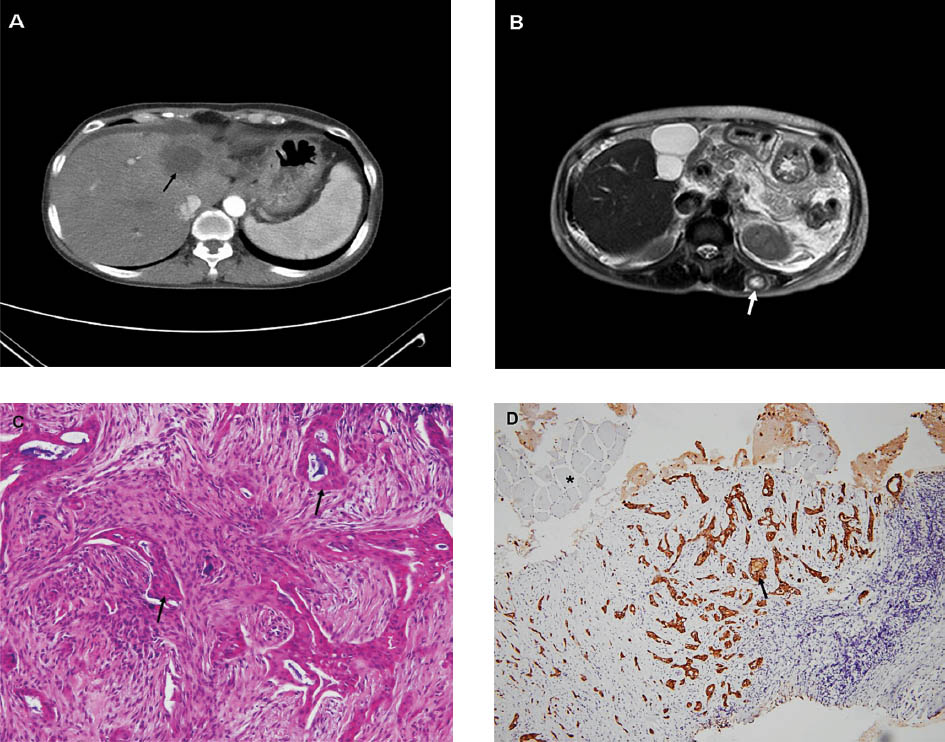
A 56 year old woman presented to the outpatient department of Internal Medicine, Tri-service General Hospital, Taipei, Taiwan, in June 2012 with left upper back soreness, swelling in lower limbs and mild dyspnoea for the past several weeks. On admission, physical examination was remarkable for malnutrition, anaemic conjunctivae and pitting oedema of both lower legs. Laboratory studies showed the following: haemoglobin, 9.4 g/dl; albumin, 2.8 g/dl; alanine aminotransferase, 81 IU/l; total bilirubin, 0.5 mg/dl; d-dimer, 6030 ng/ml; carbohydrate antigen (CA) 19-9, 5050 IU/ml; carcino embryonic antigen (CEA), 15.35 ng/ml and CA125, 860 IU/ml. Contrast enhanced computed tomography identified a hypovascular lesion in the left hepatic lobe and perihepatic ascites (Fig. A). Magnetic resonance imaging (MRI) demonstrated a nodular mass over the left longissimus dorsi muscle (Fig. B) in addition to the hepatic tumour. An ultrasound-guided biopsy was performed for the lumbar muscular tumour. Pathological analysis confirmed an adenocarcinoma (Fig. C), which was positive for cytokeratin 7 (Fig. D), but negative for cytokeratin 20, hepa-1 and thyroid transcription factor (TTF-1). Based on laboratory, imaging and histologic features, diagnosis of the intrahepatic cholangiocarcinoma with left longissimus dorsi muscle metastasis was made.
-
A Computed tomography showed a hypovascular lesion in the left hepatic lobe (arrow) and perihepatic ascites. B. Magnetic resonance imaging revealed a nodular mass over the left longissimus dorsi muscle (arrow). C. Adenocarcinoma (arrows) in muscle tissue. (hematoxylin and eosin stained 400X). D. The tumour cells were positive for cytokeratin 7 (arrow), which invaded into the normal muscle tissue (asterisk mark). (Immunohistochemical stain 100X).
Intrahepatic cholangiocarcinoma is highly invasive and usually spreads with lymphatic chains, or otherwise, intrudes adjacent structures or visceral organs12. Metastasis of skeletal muscle is a rare condition that typically involves the buttock, erector spinalis, iliacus, psoas and thorax123, and frequently presents with pain13. Therefore, muscular pain in patients with cholangiocarcinoma should raise the suspicion of metastatic disease3. A multimodality treatment approach with chemotherapy, radiotherapy, and surgical tumour debulking is usually the option for these patients. Most of patients die in less than a year from diagnosis2. Palliative radiotherapy with 45 Gy in 25 fractions was chosen for symptoms relief regarding the hepatic tumour and muscular lesion. Three-dimensional conformal radiation therapy (3DCRT) technique was selected to spare normal liver and spinal cord. Under incomplete six courses of palliative radiotherapy, the patient presented with subsided pain, but died of progressive disease one month later.
References
- Detection of distant metastasis to skeletal muscle by 18F-FDG-PET in a case of intrahepatic cholangiocarcinoma. Korean J Hepatol. 2010;16:325-8.
- [Google Scholar]
- Distant skeletal muscle metastasis from intrahepatic cholangiocarcinoma presenting as Budd-Chiari syndrome. World J Gastroenterol. 2007;13:3141-3.
- [Google Scholar]
- Rare distant skeletal muscle metastasis from hilar cholangiocarcinoma: report of a case. J Gastrointest Cancer. 2011;42:171-3.
- [Google Scholar]




