Translate this page into:
Morbidity pattern in hospitalized under five children with sickle cell disease
Reprint requests: Dr Dipty Jain, Professor, 508 Ramdaspeth, Nagpur 440 010, India e-mail: dipty47@rediffmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Children with sickle cell disease require more frequent hospital care and younger children (<5 yr of age) are more vulnerable to mortality. There are limited data on the events leading to hospitalizations and death in younger children with sickle cell disease from India. This study was, therefore, undertaken to evaluate the morbidity pattern in hospitalized under five children with sickle cell disease in a tertiary care hospital in Maharashtra, India.
Methods:
This was a prospective observational study carried out from July 2007 to June 2009. Hospitalized children below five years of age with sickle cell disease were enrolled for the study and evaluated for morbid event/s leading to hospitalization. Haematological indices were noted at baseline (most recent past when patient was not acutely sick) and at the time of hospitalization.
Results:
Eighty five children with sickle cell disease were hospitalized during the study period. Hospitalization with acute febrile illness (31%) was the most common morbid event followed by severe anaemia (30%) and acute painful events (20%). Majority (62%) of the events occurred between August and October. Forty five patients had foetal haemoglobin (HbF) more than 20 per cent (26.80±4.81%) and morbidity was significantly less in these patients.
Interpretation & conclusion:
Acute febrile illness was the most common morbid event followed by severe anaemia and acute painful event hospitalized children with sickle cell disease. There was significant seasonal variation with maximum events occurring in the monsoon season.
Keywords
Bacteraemia
children
haemoglobin
infection
morbidity
sickle cell disease

In India, sickle cell disease (SCD) is common in Vidarbha, Chhattisgarh, Madhya Pradesh, Orissa, Gujarat, Tamil Nadu and Andhra Pradesh. Contrary to the earlier belief, it is commonly seen in non tribal population in central India1. It is associated with significant morbidity and represents a major health problem in central India.
The characteristics and clinical behaviour of SCD in India are different from that in developed countries2. None of the systematic studies have documented the natural history of the disease in our country where Arab-Indian haplotype is the most common haplotype. A study similar to Cooperative study3 where a large birth cohort of SCD patients is followed regularly from the time of birth would be an ideal study to establish the natural history of the disease. However, till such a study becomes available from India, hospital based data will serve as an alternative source of information.
The need for hospital care is more frequent in children with SCD than adult SCD patients. In a study from Orissa, 42.9 per cent of SCD patients seeking hospital care were younger than 10 yr of age while 39.56 per cent of total hospitalizations of SCD patients were in the paediatric age group4. In addition, SCD children younger than five years of age, especially those between 1-3 yr of age are most vulnerable to mortality56. There are limited data on the events leading to hospitalizations and death in younger children with SCD from India. Hence, we studied the morbidity pattern in hospitalized children (<5 yr of age) with SCD.
Material & Methods
This was a prospective observational study conducted from July 2007 to June 2009 in the Department of Pediatrics, Government Medical College and Hospital (GMCH), Nagpur, Maharashtra, India. In this centre at any point of time, 10-15 per cent of total hospitalizations in paediatric wards are accounted by sickle cell disease. Children younger than five years of age with SCD (confirmed to have either homozygous SS pattern or sickle heterozygous pattern on haemoglobin analysis by cellulose acetate electrophoresis and high performance liquid chromatography) who were hospitalized for any morbid event at GMCH paediatrics ward were enrolled for the study. Assuming the prevalence of less frequently occurring morbid event (sequestration crisis) in our study was as 4.4 per cent and an alpha error of 0.05, the minimum required sample size (n) was 67 to have the study power of 80 per cent. The study was approved by the institutional ethics committee and a written informed consent was obtained from parents of all study participants.
A detailed history and clinical examination of enrolled children was done as per the pre-structured proforma of sickle cell clinic at our hospital. Haematological indices at baseline (most recent past when patient was not acutely sick) and at the time of hospitalization were noted. Of the total 85 enrolled children, 75 were previously registered in sickle cell clinic and were regularly receiving penicillin prophylaxis. Only six of the 10 unregistered patients were on penicillin prophylaxis. The remaining four were started on penicillin prophylaxis at the time of discharge from the hospital. None of the patients had received pneumococcal vaccine. Morbid events like acute painful crisis, dactylitis, severe anaemia, sequestration, acute febrile illness and stroke were defined as per standard definitions7. Only those febrile patients who were at high risk of bacteraemia8 were hospitalized.
Chi square test was used to find an association between morbid events and haematological indices. Paired t test was applied to find significant differences between haematological indices at baseline and during the event.
Results
A total of 85 children including 60 (71%) boys and 25 (29%) girls were enrolled. Infants constituted 18 per cent of the study population, while 56 per cent were younger than three years of age. Almost one third of the subjects belonged to Mahar community (32%) followed by Kunbi (20%), Gondh (20%) and Teli (13%).
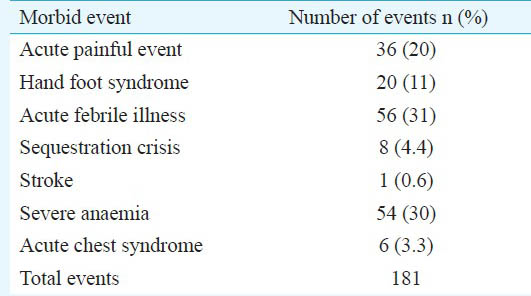
Hospitalization with acute febrile illness (31%) was the most common morbid event followed by severe anaemia (30%) and acute painful events (20%). Hand-Foot syndrome (11%), splenic sequestration crisis (4%), acute chest syndrome (3.3%), and stroke (0.6%) accounted for the rest (Table I). Morbid events like priapism, leg ulcers and avascular osteonecrosis were not seen. Two patients expired during the study period; one death was due to splenic sequestration crisis and the other was due to severe sepsis.
Common morbid events during infancy were hand foot syndrome (n=6), acute febrile illness (n=5), acute painful events (n=4) and severe anaemia (n=4) where “n” is the number of morbid events. Acute febrile illness n=56, 30.9 per cent was most commonly due to fever without focus (n=29, 52%) and osteomyelitis (n=11, 21%). Others included superficial abscess, urinary tract infection, splenic abscess and septicaemia. Bacteraemia was proved in 20 events of acute febrile illness. Staphylococcus aureus (n=8) and Gram negative bacteria (n=12) were responsible for all cases of bacteraemia. S. aureus was resistant to the first line antibiotic (oxacillin) in five (of 8) cases but most (7 of 8) were sensitive to vancomycin. Surprisingly, four (of 8) isolates were also resistant to linezolid. The isolated Gram negative bacteria included Escherichia coli (n=5), Klebsiella pneumoniae (n=5) and Pseudomonas aeruginosa (n=2). All Gram negative organisms were resistant to ampicillin and cefotaxim while nine (of 12) were sensitive to amikacin and eight (of 12) were sensitive to piperacillin-tazobactam combination. All Gram negative organisms were sensitive to imipenem.
Of the total 181 morbid events, maximum number of hospitalizations were documented in the month of August (n=42), followed by September (n=36) and October (n=34). More than half of the events (62%) were observed during the late monsoon and early post monsoon season (August to October) with least occurrence during summer (Figure).
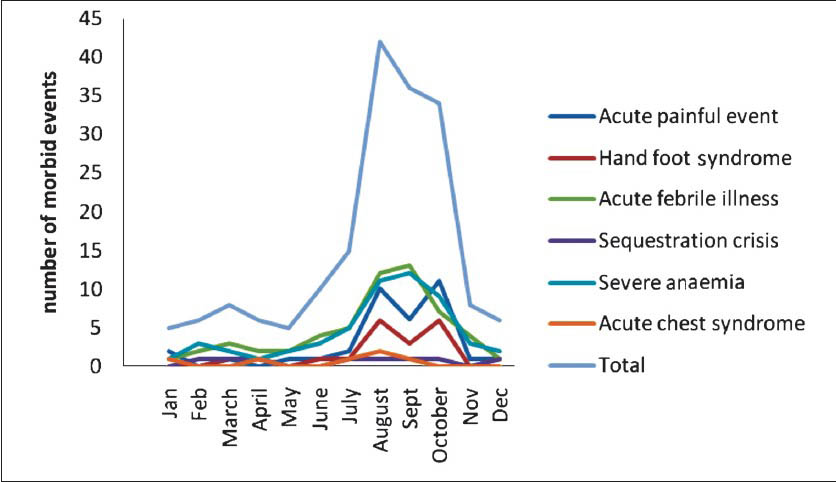
- Monthwise distribution of morbid events leading to hospitalizations. The morbid events occurred during the same months of two years of the study period are combined under the corresponding months.
The baseline haemoglobin and reticulocyte count of all study subjects were 7.41±1.61 g/dl and 3.68±1.30 per cent, respectively. Haemoglobin (7.7±1.34 vs. 7.41±1.61 g/dl; P=0.52) and reticulocyte count (4.02±1.63 vs. 3.68±1.30%; P=0.68) at hospitalization due to acute painful event were not significantly different from those at baseline. Haemoglobin during acute febrile illness (6.29±2.05 g/dl) was significantly low from baseline haemoglobin (P<0.01). The reticulocyte count during splenic sequestration crisis (7.01±2.20%) was significantly higher than that at baseline (P<0.01). In addition to eight events of sequestration crisis, 54 events of severe anaemia were documented. Among these 54 events of severe anaemia, eight were diagnosed to have aplastic crisis, while the rest were diagnosed to have haemolytic crisis. In total, 78 blood transfusions were given including 56 transfusions in 42 children with severe anaemia, seven transfusions in six children with acute chest syndrome, 11 transfusions in eight children with sequestration crisis, two transfusions in two children with sepsis with multiorgan failure and two transfusions in one child with stroke.
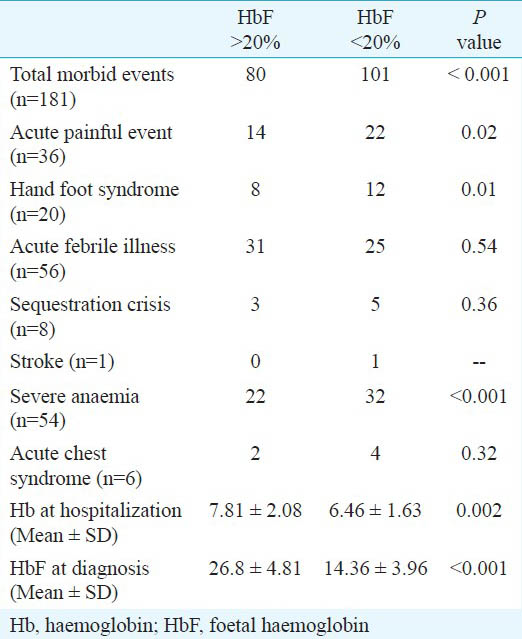
Forty five patients had foetal haemoglobin (HbF) more than 20 per cent (26.80±4.81%) while 40 patients had HbF less than 20 per cent (14.36 ± 3.96%). Total morbid events, episodes of severe anaemia, acute painful events and hand-foot syndrome were significantly more common in those with lesser HbF at baseline (Table II). Mean haemoglobin was also significantly less at the time of hospitalization in those with HbF <20 per cent.
Discussion
The present study reports morbidity pattern in hospitalized children with SCD younger than five years of age. Higher number of boys in our study (71%) was similar to other studies from central India9. Acute febrile illness was most common morbid event followed by severe anaemia. Most episodes occurred during late monsoon season. This indicates that infection is a common underlying cause for acute illness in SCD in India. Further studies should evaluate the association with viral infections. Similar to our study, infection was the most common cause of hospitalization in a Nigerian study10. This may be due to poor socio-economic status and poor hygienic conditions which predispose to infections. However, in a study from Kuwait11, vaso-occlusive crisis was the most common cause of hospitalization in SCD children. Another study from central India has reported severe anaemia requiring blood transfusion as the most common cause of hospitalization in SCD children12. In our study also, severe anaemia accounted for almost one third of the total hospitalizations. Although it was not as common as that in the Cooperative study3, children in our study also commonly had hand foot syndrome and acute painful events since infancy.
S. aureus and Gram negative bacteria accounted for all cases of bacteraemia. This finding suggests that the pattern of bacteraemia in SCD children from India may be different from that of Africa13 and Western countries3 where Streptococcus pneumoniae and Haemophilus influenzae are the most common causes of bacteremia. This difference may be due to the environmental factors, as these bacteria are also the common causes of septicaemia in children without SCD1415. This contrast may be due to use of penicillin prophylaxis also (although none of them received pneumococcal vaccine.
About 50 per cent of S. aureus isolates were resistant to the first line antibiotic (oxacillin). It may be beneficial to use vancomycin as the first line empirical antibiotic for suspected S. aureus infections and to revise the antibiotics once sensitivity patterns are available. All Gram negative organisms were resistant to ampicillin and cefotaxim and most of these were sensitive to piperacillin+tazobactam or amikacin, and also to imipenem. Hence, it may be beneficial to use the combination of amikacin and piperacillin+tazobactam as first line antibiotic therapy for suspected Gram negative infection in SCD children.
Maximum hospitalizations were seen during the late monsoon and early post monsoon season (August-October). This finding was similar to previous reports from India24. However, the studies from other countries have shown temperature16 or high wind speed and low humidity as precipitating factors for vaso-occlusive crisis in SCD subjects but not rainfall17.
Similar to a previous study from central India9, haemoglobin during painful events in our study was not significantly different from that of baseline haemoglobin. However, haemoglobin during infection was significantly low as compared to baseline haemoglobin. The mechanism for such a fall in haemoglobin during infections in children with SCD is poorly understood. However, infections may be responsible for transient bone marrow aplasia or increased haemolysis.
Similar to previous studies1819, HbF was more than 20 per cent in 45 enrolled patients. Morbid events were more common in those with HbF 20 per cent. Earlier data from India18 and Arabian countries2122 showed no significant relation between morbidity and HbF level. Another study from India23 with a large sample and prolonged follow up has shown significant negative correlation between frequency of painful crisis and HbF concentration. Strategies to improve HbF may decrease frequency of hospitalizations in SCD children. We have recently reported that use of low- fixed-dose hydroxyurea decreases hospitalization frequency in SCD children24.
This study was a hospital based study and hence, does not represent the true rate of events for SCD children in the general population. The ideal study should be a community-based cohort study or a birth cohort study.
In conclusion, in hospitalized children with SCD younger than five years acute febrile illness was the most common morbid event, followed by severe anaemia and acute painful event. Morbid events most commonly occurred during the monsoon season.
References
- Hemoglobin S and β thal: Their distribution in Maharashtra, India. Int J Biomed Sci. 2013;9:75-81.
- [Google Scholar]
- Clinical events in the first decade in a cohort of infants with sickle cell disease. Cooperative Study of Sickle Cell Disease. Blood. 1995;86:776-83.
- [Google Scholar]
- Age, sex and seasonal variations of sickle cell disorder cases in Orissa. J Hum Ecol. 1998;9:281-4.
- [Google Scholar]
- Mortality in sickle cell anemia in Africa: A prospective cohort study in Tanzania. PLoS One. 2011;6:e14699.
- [Google Scholar]
- Mortality in children and adolescent with sickle cell disease. Cooperative study of sickle cell disease. Pediatrics. 1989;84:500-8.
- [Google Scholar]
- Disorders of hemoglobin structure: sickle cell anemia & related abnormalities. In: Lichtman MA, Beutler E, Kaushansky K, Kipps T, Seligsohn U, Prachal J, eds. Williams's hematology (7th ed). New York: McGraw Hill Medical Publishers; 2006. p. :675-8.
- [Google Scholar]
- Hemoglobinopathies. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson textbook of paediatrics (18th ed). New Delhi: Elsevier Publication; 2008. p. :2026.
- [Google Scholar]
- Epidemiology of sickle cell disease in a rural hospital of central India. Indian Pediatr. 2000;37:391-6.
- [Google Scholar]
- Hospital admission of patients with sickle cell anemia pattern and outcome in Enugu area Nigeria. Niger J Clin Prac. 2007;10:24-9.
- [Google Scholar]
- Ten year review of hospital admissions among children with sickle cell disease in Kuwait. Med Princ Pract. 2008;17:404-8.
- [Google Scholar]
- Bacteraemia in Kenyan children with sickle cell anemia: A retrospective cohort and case control study. Lancet. 2009;374:1364-70.
- [Google Scholar]
- Bacterial profile of blood stream infections and antibiotic resistance pattern of isolates. JK Science. 2007;9:186-90.
- [Google Scholar]
- Windy weather and low humidity are associated with an increased number of hospital admissions for acute pain and sickle cell disease in an urban environment with a maritime temperate climate. Br J Haematol. 2005;131:530-3.
- [Google Scholar]
- Clinical diversity of sickle cell disease in western India - influence of genetic factors. Acta Hematol. 2000;103:122-3.
- [Google Scholar]
- Limitations of Hb F as a phenotypic modifier in sickle cell disease: study of Kuwait Arab patients. Hemoglobin. 2011;35:607-17.
- [Google Scholar]
- Effect of alpha thalessemia, G-6-PD deficiency and Hb F on the nature of sickle cell anemia in south - western Soudi Arabia. Trop Geogr Med. 1990;42:241-7.
- [Google Scholar]
- Higher fetal hemoglobin concentration in patients with sickle cell disease in eastern India reduces frequency of painful crisis. Eur J Haematol. 2009;83:383-4.
- [Google Scholar]
- Low fixed-dose hydroxyurea in severely affected Indian children with sickle cell disease. Hemoglobin. 2012;36:323-32.
- [Google Scholar]




