Translate this page into:
Varicella pneumonia in an adult
*For correspondence: marto.goncalo@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 35-year old man presented to the emergency room with sudden onset of fever, dyspnoea, bilateral pleuritic thoracalgy, and an exanthematous vesicular rash. He was a smoker and his two year-old son had chickenpox two weeks earlier. The patient had no previous immunization or known contact with the disease. On examination, he was febrile (39° C) with signs of respiratory distress (oxygen saturation of 88% on room air). An extensive polymorphic pruritic rash with macular, vesicles, pustules and crusty lesions was noticed (Fig. 1). Laboratory studies showed mild thrombocytopenia and elevation of liver enzymes (AST, ALT, GGT) and lactate dehydrogenese (LDH). Chest X-ray revealed multinodular interstitial infiltrates in both lungs (Fig. 2). Arterial blood gases were consistent with hypoxemic respiratory failure (PaO2 of 51.8 mmHg). HIV testing was negative. The diagnosis of varicella pneumonia with mild liver involvement on an immunocompetent patient was made and supportive treatment and intravenous acyclovir (10 mg/kg every 8 h) was promptly initiated. Excellent clinical and radiological evolution was documented, as was analytical normalization. After one week of therapy, the patient was discharged fully recovered.

- Skin examination: Polymorphic pruritic rash with macular, vesicles, pustules and crusty lesions.
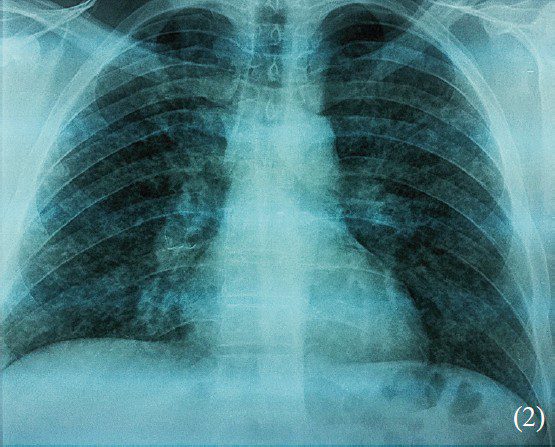
- Chest radiographic: Bilateral multinodular interstitial infiltrates.
Varicella pneumonia has an approximate incidence of 1:400 cases, being the main cause of morbility and mortality reaching up to 50 per cent in patients requiring mechanical ventilation12. Male gender2 and tobacco use3 are know risk factors. Respiratory symptoms, mainly dyspnoea and dry cough develop after a few days of rash onset, although pleuritic chest pain and haemoptysis can occur. Patients usually demonstrate progressive hypoxemia and chest radiographs reveal diffuse bilateral infiltrates. Supportive care and acyclovir are the mainstay of treatment. Mechanical ventilation, and probably steroids1 are reserved for life-threatening varicella pneumonia. The vast majority of healthy adults exibhits complete recovery4.
References
- Varicella-Zoster virus epidemiology- a changing scene? J Infect Dis. 1996;174(Suppl 3):S314-9.
- [Google Scholar]
- Outcome of varicella pneumonitis in immunocompetent adults requiring treatment in a high dependency unit. J Infect. 2001;43:135-9.
- [Google Scholar]




