Translate this page into:
Cardiac angiosarcoma discovered at a pacemaker implantation procedure
+For correspondence: County Emergency Hospital, George Cosbuc street Nr 31, 430110, Baia Mare, Romania medicbm@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 77-year old man was sent for cardiac stimulation for syncope and complete atrioventricular block at County Emergency Hospital, Baia Mare, Romania. One hour after the procedure, the patient developed diffuse thoracic pain. Chest X-ray and ecocardiography were done for right ventricular perforation suspicion. There was no lead displacement, but ecocardiography showed a 5 mm anterior pericardial effusion and right atrial and ventricular endomyocardial masses that caused tricuspid valvular obstruction with a mean pressure gradient of - 9.11 mmHg (Figs 1, 2).

- 2 D Echocardiogram showing a small pericardial effusion.
- Tricuspid Doppler flow with gradient.
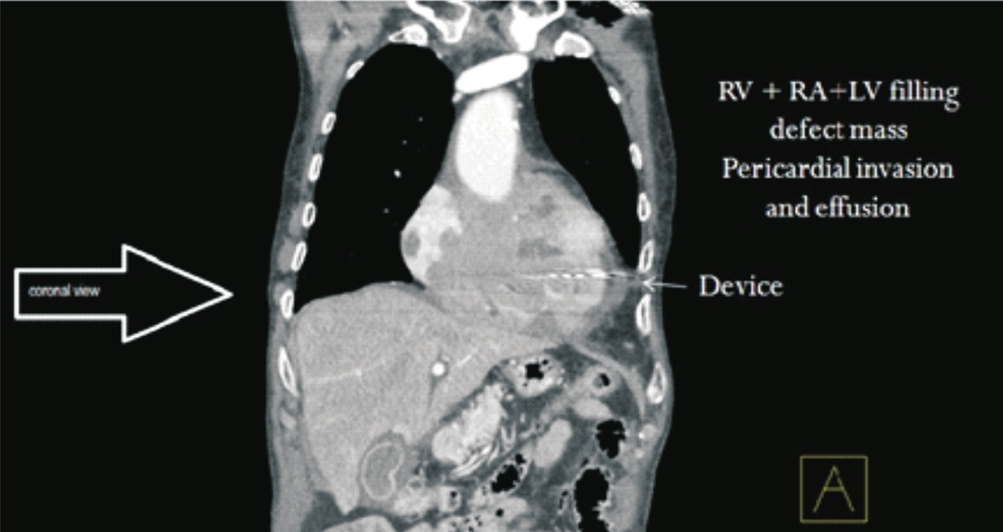
A CT-angio scanning confirmed the presence of an extensive filling defect in the right atrium and right ventricle with tricuspid valvular and right coronary ostium infiltration (Figs 3, 4). The CT image was characteristic of primary cardiac angiosarcoma. This case was one of the rare cases in whom the diagnosis was made accidental but antemortem. Histopathological confirmation was not available. Patient was only medically treated (no oral anticoagulation) and died three months later with stroke, probably embolic from angiosarcoma.
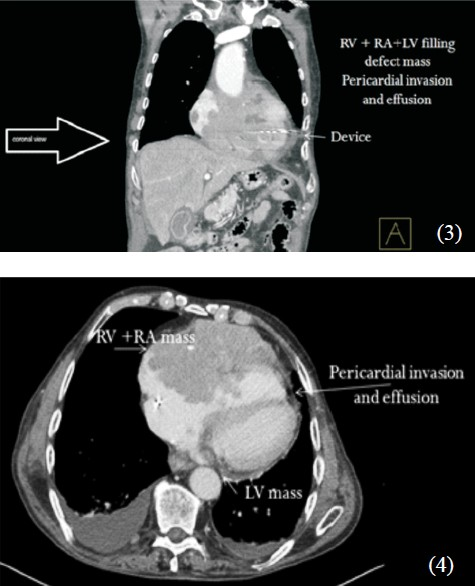
- CT angiogram with mass lesion (RV, LV, right & left ventricle; RA, LA, right & left atrium).




