Translate this page into:
Meditation as an intervention for cognitive disturbances following total sleep deprivation
Reprint requests: Dr Usha Panjwani, Scientist ‘E’ & Head, Neurophysiology Division, Defence Institute of Physiology & Allied Sciences (DRDO), Ministry of Defence, Lucknow Road, Timarpur, Delhi 110 054, India e-mail: neurophysiolab_dipas@rediffmail.com; usha_dipas@rediffmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Decline in cognitive functions is a major challenge for professionals during sustained wakefulness. We used middle latency response (MLR), event related potentials P300-ERP and contingent negative variation (CNV) and Raven's Advanced Progressive Matrices (RAPM) - a standard neuropsychological test were used to evaluate cognitive impairment after total sleep deprivation (SD); and to study the impact of meditation as an intervention for this impairment.
Methods:
Healthy male volunteers (n=10) drawn randomly from the Indian Army participated in a 6-night study design executed before and after two months of meditation practice: night 1–adaptation, night 2–baseline, night 3–24 h SD, night 4-recovery sleep, night 5–24 h SD after 60 days meditation, night 6-recovery sleep after SD. A 36 h SD was obtained by keeping the subject awake for 12 h after 24 h SD.
Results:
The latency and amplitude of P300 increased after 36 h SD. Amplitudes and latencies of both early and late CNV increased after 24 and 36 h SD, indicating deficient orientation and impairment of attention and perception. Prolonged CNV reaction time after 36 h SD manifested deficient motor response following second (imperative) stimulus. Latency of MLR Na registered significant change following 36 h SD compared to baseline (P<0.01) and recovery (P<0.05). RAPM score showed significant decrease after 36 h of wakefulness indicating impaired analytical ability and difficulty in problem solving. None of these parameters showed any significant alteration after SD, following meditation practice.
Interpretation & conclusions:
The present results showed that SD impaired cognitive performance to graded extents significantly, but this deterioration could be improved to a significant extent using meditation.
Keywords
Cognitive functions
contingent negative variation
event related potentials
middle latency response
P300
Raven's Advanced Progressive Matrices
reaction time
sleep deprivation

Several studies have depicted the effect of sleep deprivation (SD) on cognitive functions. SD is known to reduce attentional resources, thus leading to depleted error monitoring and increased errors1. It has also been evident from event related potential (ERP) studies that experimental sleep fragmentation elicits impairment in information processing capabilities associated with reduced arousal2. ERPs offer an advantage in testing cognitive functions, since the tests are reproducible, quantifiable, non-invasive objective measures of the components of cognition viz. attention, perception, reaction time, short-term memory, etc. These are cerebral scalp potentials comprising positive and negative deflections that reflect information processing of the stimulus administered3.
Most of the studies reported on cognitive impairment after SD are based on neuropsychological test performances after SD4. In very few studies event related potentials (P300 ERP and contingent negative variation, CNV) after SD have been used to assess cognitive functions. During wakefulness, long latency components of ERPs are related to attention and information processing. The best known of these components is P3005. It was reported that P300 latency was increased and P300 amplitude decreased after SD6–9. The increase in the latencies of P300 and N200 were correlated with increased sleepiness, and the increase in P200 amplitude was correlated with negative mood, anxiety, and fatigue10. Panjwani et al11 reported that early component of CNV M1 was delayed following SD. M1 is a stimulus-related frontally predominant component, reflecting the orienting response12. However, motivation incentives selectively reduce the effects of total SD on P300 latency, but that cannot attenuate the effects of SD on performance decrements in tasks that require high-level cognitive-control processes13. Partial SD does not alter the relationship between P300 and the probability and task relevance of experimental stimuli5. Although there are reports of P300 in rapid eye movement (REM) sleep, most investigators examining long latency ERPs in sleep, like Harsh et al14 found no P300 in nonREM (NREM) sleep beyond stage 115–20. These findings suggest that cognitive processing of stimulus-bound information at the level reflected by P300 ceases at some point during the transition to NREM sleep.
Despite availability of ample information on cognitive deficits following SD, there is a paucity of information regarding neuropsychological mechanisms of cognitive impairment. Meditation is a discipline by which one attempts to get beyond the conditioned, “thinking” mind into a deeper state of relaxation or awareness. Meditation has been defined as “self regulation of attention, in the service of self-inquiry, in the here and now”21. Meditation is known to have beneficial effects in psycho-somatic diseases. Previous studies from this laboratory have reported beneficial effects of meditation in hypertension, diabetes and epilepsy2223.
The present study was aimed to evaluate the efficacy of meditation as an intervention on the amelioration of cognitive decline after 24 and 36 h of SD. It was hypothesized that practice of meditation for two months would reduce the various aspects of cognitive decline including different components of memory, attention, vigilance and others as assessed by Postgraduate Institute of Brain Dysfunction (PGI), Stroop's Color World Interference (SCWI), middle latency response (MLR) and P300.
Material & Methods
The study was conducted in Neurophysiology Division of Defence Institute of Physiology & Allied Sciences (DIPAS), Delhi, from April to July 2010.
Ten healthy young male volunteers (21-30 yr) with average education level of VIII-X standard of the Indian education system (10 yr of total education) drawn randomly from the Indian Army participated in the study. They were free from any neurological disorder especially hearing loss, sleep-related and cardiac problems and diabetes. They were not taking any sort of psychotropic, psychoactive or other drugs during the course of the study and were abstained from alcohol and smoking during the experiment.
The purpose of the study was explained to them and written informed consent was obtained. The study protocol was approved by the Ethics Committee of the Institute.
Study design: The study was divided into two phases: pre- and post-intervention. A complete set of parameters comprising ERP P300, CNV, MLR and Raven's Advanced Progressive matrices (RAPM) were recorded at a fixed time in the morning (0700-0800 h) except 36 h SD (1900-2000 h). The first night was adaptation to make the subject comfortable to sleep with the necessary attachments. The first recording (baseline, BL) was performed on the morning before the same night SD, the second recording on the morning after one night's SD (24 h SD), third recording after 36 h SD (36 h SD). A 36 h total SD was obtained by keeping the subject awake for 12 h after 24 h of deprivation. Fourth recording was taken after recovery sleep (Rec SD); fifth recording after 60 days of meditation practice, on the morning of 24 h SD (Med+24 h SD). Sixth recording was performed after 36 h SD (Med+36 h SD) and seventh recording on the morning after recovery sleep (Med+Rec SD). Each volunteer slept for about 7.5 to 8 h during adaptation and baseline nights and 8.0 to 9.0 h during recovery night. The participants were allowed to play video games, watch movies, and read books according to their choice as a tool for maintenance of continuous wakefulness24.
During 36 h SD (daytime), subjects were on regular duty schedule without any extra laborious workload. This was done to assure the homogenous work pattern for them through the period of experiment with no irregular activity.
Actigraphy was performed using an Actiwatch™ (AW 64, Mini Mitter, USA) to monitor the activity profile throughout the period of experiment. The threshold activity was set such that even a nap could be detected (Actiware™ v. 5.0, Mini Mitter, USA). Activity was expressed in arbitrary units. Subjects wore the Actiwatch™ throughout the day except for the time of bathing.
Evoked potentials: Scalp was gently cleaned with NūPrep™ skin prepping gel (Weaver and Company, USA) and Ten20™ conductive EEG paste was applied to different locations on the scalp according to the internationally accepted 10–20 electrode placement system. Ag-AgCl disc electrodes (Nicolet Biomedical, USA) were used for recording. All the recordings were done with subjects in supine position and eyes open with restricted eye movements. Auditory (sound) stimulus was given to the left ear by a headphone (Telephonics, USA).
P300: Electrodes were placed at A1 and A2 (reference), Fpz (common ground), Cz and Pz (active). Two different click sounds, one non-target and the other target, were presented to the subject using standard auditory odd-ball paradigm. The subject was asked to count the rare stimuli with attention and concentration, so that he could prompt the number of clicks he had counted at the end of the session. The stimulus characteristics were - intensity: 80 dB SPL, sensitivity: 100 μV, frequency: 2 kHz, sweep pattern: gated, sweep rate: 0.9/sec, LFF: 1.0 Hz and HFF: 30.0 Hz for non-target and intensity: 80 dB SPL, sensitivity: 100 μV, frequency: 750 Hz, sweep pattern: gated, sweep rate: 0.9/sec, LFF: 1.0 Hz and HFF: 30.0 Hz target stimuli. After recording, latencies (msec) of peaks N1, P2, N2 and P300 and amplitudes (μV) of P200 and P300 were marked.
CNV: Electrodes were placed at E1 linked with E2 (eye movement), A1 (reference), Fpz (common ground), C3, C4, Cz and Fz (active). The subject worn a pair of LED goggles (Nicolet Biomedical, USA) and a headphone (for visual and auditory stimuli respectively). The subject was given two stimuli: the first ‘warning’ stimulus (S1) was auditory - a single tone sound. The subject was asked to be alert and to expect a second stimulus to come forth. After 1 sec of S1, the second ‘imperative’ stimulus (S2) was given in the form of trains of visual LED flashes and the subject was asked to press a button to stop the flash. This time was recorded as the reaction time. One single sweep was 4 sec long, and eight such sweeps were averaged for 1 set of waveforms. The entire recording consisted of 4 sets i.e, 32 sweeps. The stimulus characteristics were - intensity: 70 dB SPL, sensitivity: 2 mV, frequency: 1 kHz, sweep pattern: gated, sweep rate: 0.1/sec, LFF: 0.01 Hz and HFF: 30.0 Hz. After recording, latencies (msec) N1, and amplitudes (μV) of peaks M1 and M2 were marked.
MLR: Electrodes were placed at A1 and A2 (reference), Fpz (common ground) and Cz (active). The volunteer was instructed to concentrate towards the stimuli coming in a synchronized fashion to his left ear. The stimulus characteristics were: intensity: 75 dB SPL, sensitivity: 100 μV, frequency: 500 Hz, sweep pattern: gated, sweep rate: 39.1/sec, LFF: 10.0 Hz and HFF: 100.0 Hz. Latencies (msec) of peaks Na and Pa and amplitude (μV) of Na - Pa were marked.
Psychological assessment
RAPM: This was done in a calm, quiet environment. Subjects were explained the modality of the test in detail and asked to practice with set-I accordingly. Each problem page (in both sets) contained nine design cells displayed in a square manner of 3 by 3 (a matrix), with the bottom-right cell vacant. The design pattern followed a particular trend across the rows and down the columns. The subjects had to predict the possible design pattern for the vacant cell and choose the same from a list of eight patterns provided below the matrix. There was no time restriction for solving the practice set. After completing set-I, they were asked to solve the matrices in the set-II (actual test set) within a time frame of 30 min. The reason for time-locking was to make the subject more attentive towards the test.
This was a 25 min session of spiritual exercise performed by moderate workers on a twice daily basis for 60 days. Each session consisted of four stages with volunteer sitting in upright position and back erect - first quietly with eyes closed for 6 min. This was followed by the Pranayama “Udgeet” - the respiratory exercise for the next 6 min, in which the volunteer sat with hands in upright position and mouth shut. The index finger was placed on the forehead; with next three fingers covering his eyes and the thumb pressing the ear lid. This is to ensure blockage of energy exchange with the universe except through respiration. In this state the person chanted ‘mmmm’ of the ‘Om’ with slow deep breathing. Next 6 min the ‘Om’ was chanted while sitting erect on back and exhaling slowly with the eyes closed. Last 6 min were spent in absolute stillness, wherein the volunteer sat with eyes closed and breathing slowly, again in first posture. At the end, participants raised their hand above their head, rasped the palms first slowly, and then briskly, placed the palms over the eyes and the session was completed.
Statistical analysis: Statistical analyses were done using SPSS 13.0 (IBM, USA). Analysis of statistical significance for changes during various conditions was performed using one way ANOVA for repetitive measurements for CNV, P300-ERP and MLR. Each value at a given condition was compared to that in another condition using multiple comparison (post hoc) t-tests. RAPM was analyzed using Friedman's rank test for analysis of significant difference within groups, followed by Mann Whitney's U test to analyze between group significance. Pearson's product-moment correlation coefficient (r) was computed to see for significant correlation between RAPM with MLR-Na, P300-P3, P300-P3 amplitude (AMP), CNV-M1, CNV-M1 AMP, CNV-M2 and CNV-M2 AMP. The determined r was then converted to Student's t-scores for testing of Ho (significance).
Results
Effect of SD on cognitive performance
Evoked potentials:
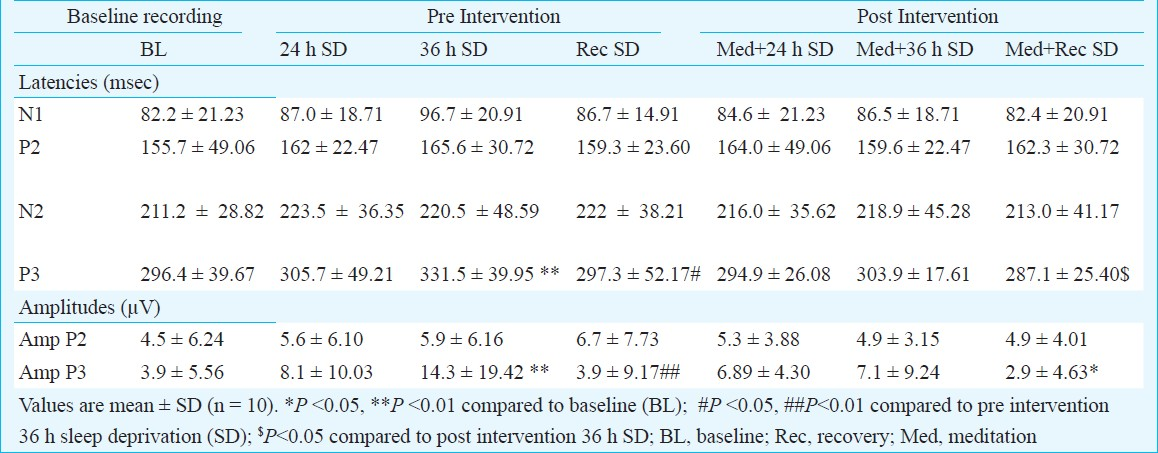
P300: N1, P2 and N2 components of P300 ERP did not register any significant change, though there was increase in latencies after 24 and 36 h of SD. Latency of P300 registered significant increase after 36 h SD (Table I) compared to baseline (P<0.01), and significant reduction was noted after recovery sleep (P<0.05). Amplitude of peak P2 did not register any significant change. Amplitude of P300 component increased following 24 h SD as well as 36 h SD (P<0.01), and returned to its baseline range after recovery sleep (P<0.01) (Table I).
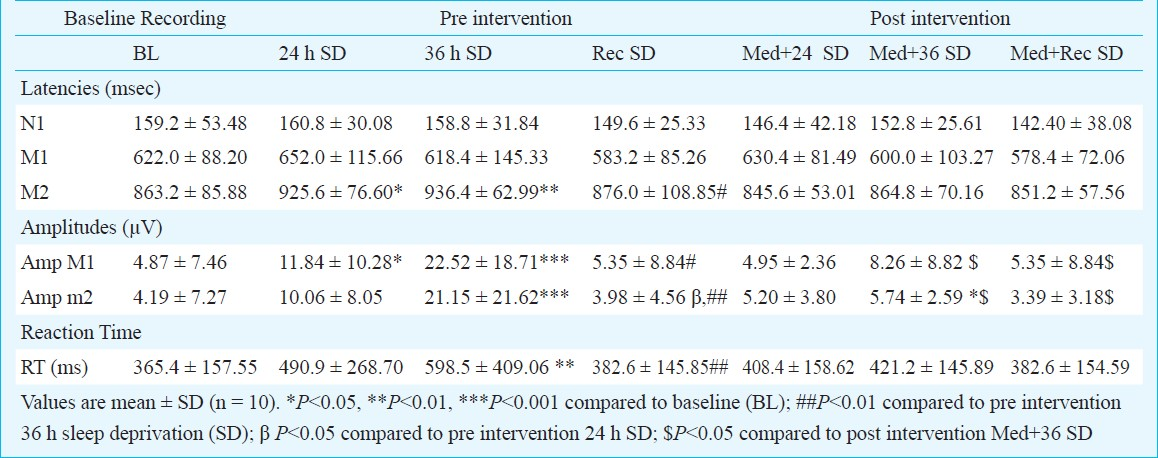
CNV: Latencies of N1 and M1 did not alter significantly. However, M2 was delayed significantly after 24 h SD (P<0.05) and the delay was greater after 36 h SD (P<0.01) compared to baseline (Table II). The latency returned to baseline after recovery sleep (P<0.05, recovery compared to 36 h SD). Amplitudes of CNV revealed significant changes with different degrees of SD. Amplitude of M1 increased after 24 h SD significantly (P<0.05), which was even higher following 36 h of prolonged deprivation (P<0.001), compared to baseline. After recovery sleep, there was significant reduction in the amplitude of M1 compared to 36 h SD (P<0.05). Amplitude of M2 showed significant elevation after 36 h SD (P<0.001) compared to baseline. After recovery sleep, significant reduction in amplitude of M2 was observed compared to both 24 h (P<0.05) and 36 h (P<0.001) of SD (Table II). In comparison to baseline, CNV reaction time was prolonged following 24 and 36 h of SD, the latter being significant (P<0.01). After recovery sleep, reaction time again registered significant decrease compared to 36 h SD (P<0.01).
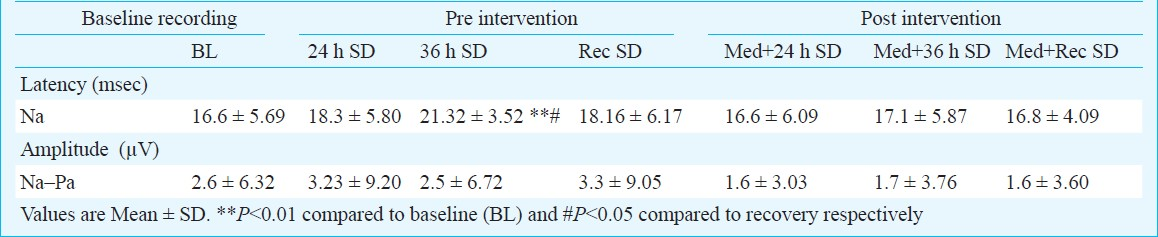
MLR: Latency of the peak Na registered no significant change after 24 h SD but significant change following 36 h SD compared to baseline (P<0.01) and recovery (P<0.05). Latency of Pa and amplitude of Na - Pa did not register any significant change at any stage (Table III).
Psychological assessment: Total SD decreased number of correct responses in RAPM set-II session after 24 h and 36 h (P<0.01) compared to baseline. This decline was recovered (P<0.01, compared to 36 h SD) after recovery (Fig.). Number of correct responses in RAPM set-II session showed significant negative correlation with amplitude of M1 component of CNV (r = -0.66; P<0.05) at baseline. No significant correlation was found between RAPM and other components viz. MLR-Na, P300-P3, P300-P3 AMP, CNV-M1, CNV-M2 and CNV-M2 AMP.
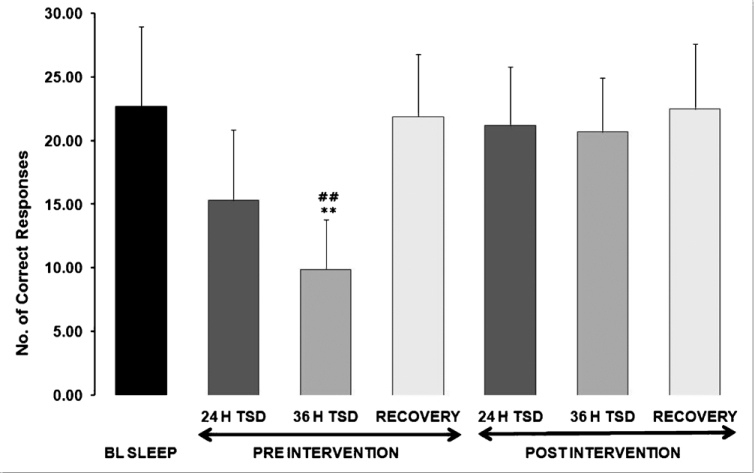
- Effect of meditation practice on number of correct responses in RAPM after sleep deprivation.
Effect of meditation as an intervention
P300: As shown in Table I (and also in Fig. 1), P300 ERP registered no significant changes in terms of latencies of N1, P2, N2 and P300 components. However, latency of P300 was decreased after recovery sleep. Amplitude of peaks P200 and P300 did not register any significant change. There was significant reduction in amplitude of P300 (P<0.05) after recovery sleep.
CNV: There was no significant change in latencies of N1, M1 and M2 components of CNV (Table II). Amplitude of M1 also did not alter significantly, though there was a significant increase in M2 amplitude after 36 h SD (P<0.05). However, this increase was ameliorated after recovery sleep.
MLR: After two months of meditation practice, there was no significant change in any components of MLR (Table III).
Neuropsychological assessment: Total SD slightly decreased number of correct responses in RAPM set-II session after SD compared to baseline (Fig.). This decline was recovered after recovery sleep. No significant correlation was found between RAPM and CNV, P300 ERP and MLR.
Discussion
The present study used a novel approach to evaluate the psychophysiological and functional measures of cognition together. The study also attempted to establish the relationship between the psychophysiological components i.e. RAPM scores with the latencies and amplitudes of P300, CNV and MLR.
In our study P300 component of ERP showed significant increase after 36 h of SD in terms of latency. This is indicative of reduced ability of concentration, discrimination of a target stimulus in a train of non-target stimuli; matching the stimulus against the memory representation of the relevant (target) stimuli and decision making (whether the presented stimulus is a target one). P300 is elicited when a form of selective attention is required by the subject in order to identify infrequent occurrences of a target (relevant) stimulus, which is presented unpredictably24. The delayed P300 latency also indicates that there is improper classification and recognition of stimulus as relevant to the assigned task. Our study was in conformity with those of earlier studies71025. Lee et al10 have reported significantly prolonged latency of N2 and decreased amplitudes of N1, P200 and P300. In our study delay in latencies of N1, P2 and N2 components of this ERP was found but not significant. N1 and N2 components are related to sensory processing of a stimulus26. N2 preceding P300 may directly affect the absolute timing of decision processes in sensory discrimination; and it is also sensitive to the cognitive attributes to the stimulus27. Amplitude of P300 increased after 24 and 36 h SD, the latter being significant compared to baseline. This was in contrast to the earlier studies710. P300 amplitude depends upon the selective attention of a subject, which is compromised after SD. Unexpected events invariably elicit larger P300 waves than do predictable events. After SD a person gets inattentive to a considerable extent which results in unpredictable presentation of a predictable stimulus. Another possible explanation may be that, stimuli which signal some internal response (like memory task in P300) or provide useful information (like target and non-target discrimination criterion in P300), result in an ERP component (like P300) with definitely higher amplitude24. After 24 and 36 h SD, the components of discrimination would be affected.
CNV appears to represent the summation of at least two, probably more, component waveforms. One previous study has reported increase in amplitude of CNV components after 24 h SD in epileptics28 as found in our study. In our study, the early component of CNV (M1) was delayed non-significantly following SD. M1 is a stimulus related frontally predominant component, perhaps reflecting the orienting response. On the other side, M2, the late CNV component is a centrally predominant component thought to be related to the premotor potential associated with the motor response29. A delayed M1 indicates subject's deficient ability to get ‘warned’ after the warning stimulus (S1) and to get ‘oriented’ about S1 as well; and delayed M2 indicates improper preparation for the subsequent motor response. Latency of M2 was significantly increased following 24 h SD and 36 h SD compared to baseline. This reveals an impaired expectancy toward S2. A significantly prolonged reaction time implies a state of deficient motor response, subject's incapability of perceptual processing and preparatory judgment.
MLR reported significant increase in latency of Na. Na is believed to be generated subcortically and Pa, bilaterally within the primary auditory cortex30. After continuous wakefulness, the conduction at the subcortical level may be delayed; or there may be some changes, which appear to resemble changes in Na latency after subcortical lesion. The reversal of the situation after recovery sleep i.e., reduction of Na latency after recovery sleep proposes that, the effect of prolonged wakefulness is ameliorated by 8-9 h of recovery sleep. In humans mid latency responses may actually consist of overlapping potentials originating from primary auditory cortex, ascending activating system and/or subcortical structures31. It is possible that SD may lead to changes in neural processing at some or all of these levels. As mentioned earlier23, MLR has got some attention related cortical components, which may deteriorate after SD.
RAPM measures two main components of intelligence; the ability to think clearly and make sense of complexity known as ‘eductive ability’, and the ability to store and reproduce information called ‘reproductive ability’32. It appears to measure a type of reasoning ability with very high predictive validities in most occupational groups. So far there is no study showing these cognitive measures using RAPM after SD. We found severe deterioration in number of correct responses after 36 h SD. It may be posible that 36 h SD interferes with educative and reproductive ability, which leads to deficient problem solving and analytical ability.
The educative and reproductive abilities involve important components of cognitive function like attention, vigilance, concentration and working memory. It was therefore, not surprising that a significant negative correlation was obtained between the amplitude of M1 (early CNV) and number of correct responses in RAPM set-II. A plausible explanation for this effect is that, following SD, a greater effort in terms of trying to concentrate harder is needed for the same extent of task complexity. The greater amount of subjective effort is reflected in increased M1 amplitude and the poor performance is depicted by reduced RAPM scores.
In conclusion, the present study validates and extends the value of P300, CNV and MLR as the markers for quantification of the degree of cognitive impairments after total SD. It also shows that total SD involves deficit in sensory perception as well as inefficiency in motor responses, which leads to cognitive impairment in an integrative manner, as is evident from significant changes in P300, CNV, MLR and RAPM scores. Thus, cognitive impairment after total SD is an assembly of dysfunctions in different regions of brain rather than being a single component; and the event related (P300 and CNV) and evoked potentials (MLR) can analyze the situation real-time, which is further confirmed by RAPM scores, the psychophysiological assessment tool.
Acknowledgment
This research was supported by fund from Defence Institute of Physiology and Allied Sciences (DIPAS), DRDO (Ministry of Defence, GOI). The authors thank the volunteers for their unstinted cooperation during the course of experiment. The authors also thank Dr Y.K. Sharma, Scientist ‘E’ for statistical analysis of data, and Shri Hempal Punia (Yoga Trainer from Defence Institute of Psychological Research, DRDO) for the meditation training of the participants.
References
- Waking quantitative electroencephalogram and auditory event related potentials following experimentally induced sleep fragmentation. Sleep. 2003;26:687-94.
- [Google Scholar]
- The recording and analysis of event related potentials. In: Boller F, Grafman J, eds. Handbook of neuropsychology. Vol x. Elsevier BV; 1995. p. :3-73. Sect. 14
- [Google Scholar]
- Effects of sleep loss on team decision making: motivational loss or motivational gain. Hum Factors. 2007;49:646-60.
- [Google Scholar]
- P300 and sleep related waveforms (P220, P450 and P900) have different determinants. J Sleep Res. 2001;10:9-17.
- [Google Scholar]
- The effect of 24-40 hours of sleep deprivation on the P300 response to auditory target stimuli. Aviat Space Environ Med. 2007;78(Suppl 5):B216-23.
- [Google Scholar]
- The P300 event related potential. The effects of sleep deprivation. J Occup Med. 1992;34:1143-52.
- [Google Scholar]
- Auditory evoked potentials as a function of sleep deprivation. Work Stress. 1989;3:79-91.
- [Google Scholar]
- Influence of extended wakefulness on automatic and nonautomatic processing. Hum Factors. 1994;36:652-69.
- [Google Scholar]
- Auditory event related potentials and psychological changes during sleep deprivation. Neuropsychobiology. 2004;50:1-5.
- [Google Scholar]
- Electrophysiological correlates of cognition improve with nap during sleep deprivation. Eur J Appl Physiol. 2010;108:549-56.
- [Google Scholar]
- Impact of monetary incentives on cognitive performance and error monitoring following sleep deprivation. Sleep. 2010;33:499-507.
- [Google Scholar]
- ERP and behavioral changes during the wake/sleep transition. Psychophysiology. 1994;31:244-52.
- [Google Scholar]
- Brain processing of stimulus deviance during slow-wave and paradoxical sleep: a study of human auditory evoked responses using the oddball paradigm. J Clin Neurophysiol. 1995;12:155-67.
- [Google Scholar]
- The effects of varying stimulus intensity on P300 during REM sleep. Neuroreport. 1999;10:2313-8.
- [Google Scholar]
- Endogenous components of event-related potential appearing during NREM stage 1 and REM sleep in man. Int J Psychophysiol. 1994;17:165-74.
- [Google Scholar]
- ‘Oddball’ event-related potentials and information processing during REM and non-REM sleep. Clin Neurophysiol. 1999;110:53-61.
- [Google Scholar]
- Information processing and coping style during the wake/sleep transition. J Sleep Res. 1998;7:225-32.
- [Google Scholar]
- Auditory event-related potentials to deviant stimuli during drowsiness and stage 2 sleep. Electroencephalogr. Clin Neurophysiol. 1995;96:398-412.
- [Google Scholar]
- Meditation, melatonin and breast/prostate cancer: hypothesis and preliminary data. Med Hypotheses. 1995;44:39-46.
- [Google Scholar]
- Effect of Sahaja Yoga practice on seizure control and EEG changes in patients of epilepsy. Indian J Med Res. 1996;103:165-72.
- [Google Scholar]
- Effects of Hatha yoga and Omkar meditation on cardiorespiratory performance, psychologic profile and Melatonin secretion. J Altern Compl Med. 2004;10:261-8.
- [Google Scholar]
- Less effective executive functioning after one night sleep deprivation. J Sleep Res. 2005;14:1-6.
- [Google Scholar]
- Cognitive functions and event related brain potentials. In: Nodar RH, Barber C, eds. Evoked potentials II, The second international evoked potentials symposium (Chap 5). MA USA: Butterworth; 1984. p. :58-9.
- [Google Scholar]
- Cognitive deterioration and changes of P300 during total sleep deprivation. Psychiatr Clin Neurosci. 2003;57:490-6.
- [Google Scholar]
- Cognitive performance and event related brain potentials under simulated high altitudes. J Appl Physiol. 1993;74:1735-41.
- [Google Scholar]
- Manipulation of event-related potential manifestations of information processing stages. Science. 1982;218:909-11.
- [Google Scholar]
- Changes in evoked slow cerebral potential (contingent negative variation) in epilepsy. Korsakov J Neurol Psychiatr. 1998;98:35-9.
- [Google Scholar]
- Effect of cortical lesions on middle latency auditory evoked responses (MLR) Electroenceph Clin Neurophysiol. 1987;66:108-20.
- [Google Scholar]
- Possible overlapping potential of the auditory P450 in humans: Factor analysis of middle latency auditory evoked potentials. Electroenceph Clin Neurophysiol. 1997;104:23-30.
- [Google Scholar]




