Translate this page into:
Whole cell & culture filtrate proteins from prevalent genotypes of Mycobacterium tuberculosis provoke better antibody & T cell response than laboratory strain H37Rv
Reprint requests: Dr. Beenu Joshi, Scientist E, Department of Immunology, National JALMA Institute for Leprosy & Other Mycobacterial Diseases (ICMR), Taj Ganj, Agra 282 001, India e-mail: bjjalma@gmail.com beenuj2002@yahoo.co.in
-
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The immune responses to different antigens of Mycobacterium tuberculosis H37Rv vary from patient to patient with tuberculosis (TB). Therefore, significant difference might be documented between the H37Rv with long histories of passages and recent clinical isolates of M. tuberculosis. In the present study, immune response of TB patients and healthy controls against 39 clinical M. tuberculosis isolates was correlated with laboratory strain H37Rv.
Methods:
The antibody response was studied coating whole cell extracts and culture filtrate proteins of M. tuberculosis isolates and laboratory strain H37Rv by enzyme linked immunosorbent assay (ELISA). Lymphoproliferation was studied by incorporation of tritiated thymidine and cytokines (IFN-γ and IL-4) by using commercially available kits.
Results:
Sero-reactivity to whole cell extract (WCE) of 11 clinical isolates was higher with pooled serum and individual's serum from tuberculosis patients showed significant reactivity (P<0.05) to ten of these isolates using ELISA. Of the WCE of 39 clinical isolates, 10 were found to be potent inducer of lymphoproliferation as well as cytokine secretion (P<0.05) in peripheral blood mononuclear cells from PPD+ healthy controls. Six culture filtrate proteins (CFPs) from these selected clinical isolates were also better inducers of antibody and T-cell response.
Interpretation & conclusion:
Overall, our results revealed that the clinical isolates belonging to prevalent genotypes; CAS1_Del (ST-26), East African-Indian (ST-11) and Beijing family (ST-1) induced better antibody and T cell responses compared to H37Rv laboratory strain. Further studies need to be done to purify and identify the dominant protein (s) using whole cell extract and culture filtrates from these immunologically relevant clinical M. tuberculosis isolates, which will be worthwhile to find out pathogenic factors, potential diagnostic markers and protective molecules for tuberculosis.
Keywords
Antibody and cell mediated response
culture filtrate protein
clinical Mycobacterium tuberculosis isolates
whole cell extract

Tuberculosis (TB) continues to remain as one of the major killer contagious diseases with nearly 1.7 million deaths and more than 9.4 million new cases each year1. Early and specific diagnosis is essentially required for control of disease. The development of specific immuno-diagnostic tests for tuberculosis has been hampered by cross-reactive antigenic epitopes of M. tuberculosis between different mycobacterial as well as with other non mycobacterial strains2. Cross-reactivity of most of the M. tuberculosis antigens with BCG further complicates the immune based diagnosis of tuberculosis34 as most of the people are BCG vaccinated especially in the endemic country like India.
Immune-based tests are known as the valuable tool to diagnose a disease during early phases of the infection. Several investigations have been done to develop a sensitive and specific immuno-diagnostic assay by extracting the antigens from M. tuberculosis strain H37Rv, but these assays suffer from variable immune responses5. H37Rv is maintained in the laboratories from a long time by in vitro passages, and therefore, appear to have lost its high virulent factors and may be immunodominant antigens. Recently, it has been shown that two closely related M. tuberculosis Beijing isolates collected in South Africa have vastly different pathogenic characteristics in terms of their ability to transmit and cause disease in humans and to cause pulmonary damage in mice6. Therefore, systematic studies in different regions are needed to map the antigen profile of M. tuberculosis isolates from patients with TB to understand the relationship between antigenic feature of M. tuberculosis with the prevailing epidemiological situation. In India, being a high incidence country, features of M. tuberculosis bacilli may be distinct from place to place, which suggest an urgent need to search for dominant antigens from prevalent strains of M. tuberculosis present in the community, these antigens could be used as a diagnostic or vaccine candidate (s).
Therefore, this study was designed to evaluate the immune-reactivity of clinical isolates of M. tuberculosis obtained from different regions of India in comparison to laboratory strain H37Rv using enzyme linked immunosorbent assay (ELISA), lymphoproliferation assay and cytokine estimation.
Material & Methods
M. tuberculosis clinical isolates: Thirty nine clinical M. tuberculosis isolates from ten different regions of India (Agra, Kanpur, Delhi, Ranchi, Karnataka, North East, Jaipur, Ahamedabad, Allahabad and Bhopal) and laboratory strain H37Rv were collected from Mycobacterial Repository Centre of National JALMA Institute for Leprosy and Other Mycobacterial Diseases, Agra, India. The isolates were arbitrarily selected in terms of geographical source and growth profile. These isolates were inoculated (108 cfu/ml) in tween-80 free Sauton's medium on a shaking incubator at 37°C.
Spoligotyping of clinical isolates: DNA from M. tuberculosis isolates was extracted by the method of van Embden et al7. Spoligotyping to detect 43 spacers was done using commercially available kit (Ocimum Biosolutions, Hyderabad) as described previously8. Binary format results were converted into octal code and compared with the international Database SpolDB4.09. Spoligopatterns not found in SpolD4.0 were analyzed with “Spotclust”10.
Preparation of whole cell extracts (WCE): M. tuberculosis growth was collected from Sauton's medium by centrifugation at 10,000×g and washed twice with 150 mM phosphate-buffered saline (PBS, pH 7.4). The growth was suspended (0.2 g growth/ml) in PBS and extraction buffer (50 mM Tris buffer, 10 mM MgCl2, 1 mM ethylene glycol tetra-acetic acid, 1 mM phenylmethylsulphonyl fluoride, pH 7.4). Bacteria were sonicated with a vibra cell probe ultra-sonicator for a total of 20 min using 50 per cent output control (100%=475 w) and 50 per cent duty cycle (on/off) at 4°C11. WCE were collected by centrifugation at 23000×g for 30 min. The protein concentration of each cell extract was estimated using the Bradford's method12. These extracts were stored at -20°C till used.
Preparation of culture filtrate proteins (CFP): M. tuberculosis bacilli were removed and resultant culture filtrate was processed as described earlier13. Briefly, culture filtrate was sequentially filtered through 0.45 μm followed by 0.22 μm Millex GV PVDF membrane (Millipore, Bedford, MA, USA). SDS (10%) (Sigma, USA) was added to obtain 0.1 per cent final concentration (w/v) in the culture filtrate (CF) and kept in a boiling water bath for 5 min. CF was treated with trichloroacetic acid (TCA) (Sigma, USA) to obtain final concentration 10 per cent (w/v). Finally, this mixture was incubated at -20°C for 5 h and the resulting precipitate was removed by centrifugation at 18,000×g for 30 min at 4°C. Minimum volume of HPLC grade water (Qualigens fine chemicals, Mumbai, India) was added to disperse the pellet and then the whole suspension was washed with 1 ml of pre-chilled acetone (Sigma, USA). Air dried pellets were dissolved in minimum volume of 2D rehydration buffer (Bio-Rad Laboratories, Hercules, CA, USA). CFP for cell proliferation assays were prepared by buffer exchange method using PBS. The protein concentration was determined by Bradford's method12.
Study subjects: Serum samples from HIV negative tuberculosis patients (n=55, age range 18 to 60 yr) were collected from State Tuberculosis Demonstration Centre (STDC) and Department of Tuberculosis & Chest Diseases (TBCD), S. N. Medical College, Agra, India. All these patients were clinically diagnosed as pulmonary TB and confirmed bacteriologically by staining for acid fast bacilli/ isolation of tuberculous bacilli in cultures of Lowenstein-Jensen medium. These patients were categorized into three clinical groups (35 active untreated TB, 10 defaulter TB and 10 relapsed TB cases) as per the guidelines of Revised National TB Control Program, Central TB Division, Government of India14. Six samples from individuals who were taking standard treatment for TB for more than 5 months were also included in this study.
Serum samples from healthy controls (n=21) were collected from students (age range 18-25 yr) working in Immunology laboratory for short term projects of the Institute. Ten confirmed lepromatous leprosy (LL) controls were also included from out patient department (OPD) of National JALMA Institute for Leprosy and Other Mycobacterial Diseases (ICMR), Agra. All serum samples were collected and stored at -20°C until used. The study was approved by Institutional ethical committee and informed consent was obtained from each patients.
Pooled serum preparation: Equal volume of 10 serum samples was pooled separately from different categories of individuals. (i) HPS (healthy subjects pooled serum); healthy BCG vaccinated subjects. (ii) FPS (fresh/new TB cases pooled serum); patients who had infection with M. tuberculosis for the first time and had no history of tuberculosis treatment. (iii) DPS (defaulter TB cases pooled serum); patients who had not taken the complete course of anti-tubercular treatment and the symptoms re-occurred. (iv) RPS (relapsed TB cases pooled serum); TB patients who were treated earlier for TB but symptoms re-occurred after completion of the treatment. (v) TPS (treated TB cases pooled serum); individuals who were taking standard treatment of TB for more than 5 months. (vi) LLPS (lepromatous leprosy cases pooled serum); confirmed lepromatous leprosy (LL) patients.
Enzyme linked immunosorbent assay (ELISA): ELISA was performed using standard protocols as described previously15. Briefly, maxisorp ELISA plates (Nunc Maxisorp, Roskilde, Denmark) were coated with 100 μl of 125 ng/ml whole cell extract/culture filtrate protein of clinical isolates and H37Rv in carbonate bicarbonate (0.05 M, pH 9.6) buffer per well. The plates were read at 492 nm using an ELISA reader (Spectramax-M2 Reader, Molecular Devices, Sunnyvale, CA, USA).
T-cell proliferation assay: Peripheral blood mono-nuclear cells (PBMCs) were separated from heparinized blood of healthy individuals (10 individuals for WCE and 6 for CFP) by density gradient centrifugation over Ficoll hypaque16. The washed cells were counted and adjusted to 1×106 cells / ml in culture medium (RPMI 1640) and dispensed (100 μl/well) into 96 well flat bottom culture plates (Nunc, Roskilde, Denmark). Culture were set in triplicate with or without antigen in culture medium (100 μl/well) containing 5 per cent heat inactivated foetal calf serum supplemented with 2 mM L-glutamine and antibiotic & antimycotic and incubated for 5 days in a CO2 incubator. Purified protein derivative (PPD) was taken as positive control in each experiment. Optimum doses (10 μg/ml for WCE and 1 μg/ml for CFP) for proliferation responses were determined by adding increasing amounts of WCE and CFP from clinical isolates at concentrations ranging from 1 to 25 μg of protein per ml to PBMCs (1×106 cells/ml) suspension. The culture was pulsed with 3H-thymidine (1 μci/well) for 18 h before harvesting, and the radioactivity of the harvested cells was measured in a β-liquid scintillation counter (LKB Rackbeta, Finland).
Cytokine ELISA: The culture supernatants from PBMC culture were harvested after 5 days of incubation in a CO2 incubator and stored at -20°C until use. Cytokine (IFN-γ & IL-4) levels were estimated by using e-Bioscience cytokine detection kit (San Diego, USA) according to the manufacturer's instructions.
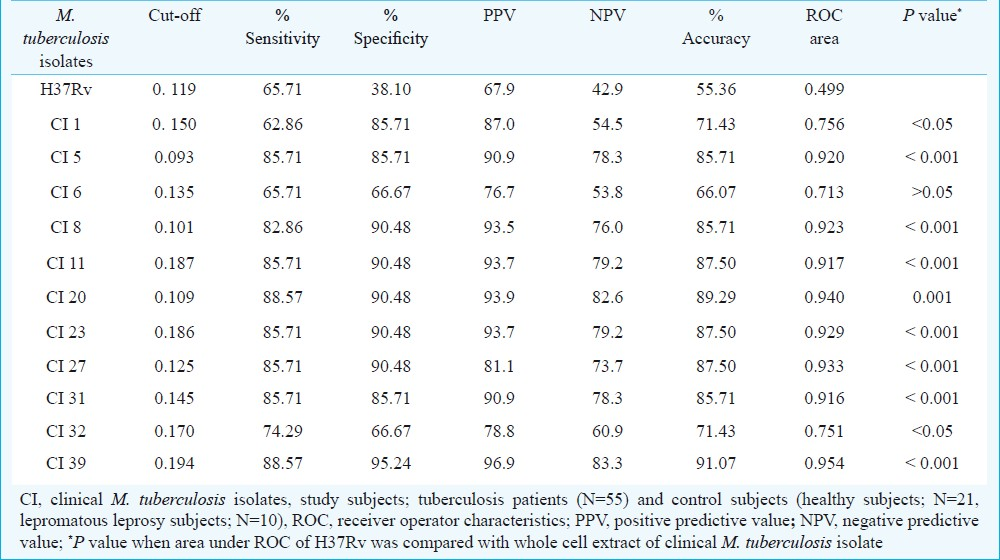
Statistical analysis: Cut-off value, sensitivity and specificity for each antigen against individual serum were calculated by ROC (receiver operator characteristics) analysis using software STATA-7 (Strata Corporation, College Station, TX, USA). The cut-off was selected at the point which showed the best accuracy (correctly classifying individuals to their groups), sensitivity, and specificity by ROC. A positive predictive value (PPV) is defined as the probability to characterize a patient for the particular disease from the patient's population, and negative predictive value (NPV) is also needed to exclude the disease. Scattergram was plotted using GRAPHPAD software prism version 5.0 (GraphPad Software, Inc., San Diego, CA, USA).
T-cell proliferation response of stimulated PBMCs was defined as stimulation index (SI) which was calculated by dividing the mean counts per minute (CPM) of experimental wells by mean CPM of control wells. T-cell proliferation and cytokine response was correlated and Spearman correlation coefficient (r) was calculated.
Results
Serological response of whole cell extracted and culture filtrate proteins: High optical density (>2 times) was observed using pooled serum from TB patients and low optical density taking pooled serum from lepromatous leprosy against total 22 clinical M. tuberculosis isolates (CI1,5,6,8,9,10,11,12,13,15,16,19,20,22,23,24,25,27,31,32,33 and 39) in comparison to healthy subjects (data not shown). Finally, total eleven clinical isolates (CI1,5,6,8,11,20,23,27,31,32 and 39) representing eight different regions were selected for further serological analysis using individual serum from different types of tuberculosis cases (Fig. 1A, Table I). Overall antibody reactivity of TB patients’ serum samples against 10 clinical isolates was significantly greater than healthy controls, however, reactivity was not significant against CI6 and M. tuberculosis H37Rv (Table I). Sensitivity was highest (88.57%) with WCE of CI20 and CI39 followed by CI5, CI11, CI23, CI27, CI31 (85.71%), CI8 (82.86%) and CI32 (74.29%) as compared with H37Rv (65.71%). Similar reactivity to CI6 was noted as H37Rv, and CI1 (62.86%) was comparatively less reactive. Accuracy of ELISA was high to all clinical M. tuberculosis isolates and it was 55.36% for H37Rv (Table I). All the clinical isolates showed higher reactivity in fresh tuberculosis cases than H37Rv except CI1, and CI6 (Fig. 1A). Highest reactivity (80%) to defaulter tuberculosis cases (DTB) was noted against CI39 and slightly higher antibody (60%) was reported against CI5, CI8, CI11, CI20, CI23, CI27, CI31 and CI32 as compared with H37Rv (40%). Reactivity to clinical isolate1 and 6 was only 50 per cent in DTB group of patients. The reactivity to treated cases was highest (100%) against CI20 and to all other clinical isolates was 83.3 per cent except CI1 (50%). Only 50 per cent treated TB cases were reactive when antibody was detected against H37Rv. The reactivity to serum from lepromatous leprosy patients was highest (100%) against WCE of CI5, CI20, CI23, CI27, and CI31 followed by 90 per cent for CI32 and CI39. Lowest reactivity (70%) was observed for CI1, CI6, and CI11. The reactivity against H37Rv was found 80 per cent with leprosy patient.
![(A): Scatter diagram of IgG antibody response to whole cell extract from various selected clinical isolates with individual serum from different groups of patients [patients with fresh pulmonary tuberculosis (PTB), defaulter TB (DTB), relapse TB (RTB), treated TB (TtTB), and lepromatous leprosy patients (LP)] and controls (HS, healthy subjects) (b-l) in comparison with M. tuberculosis H37Rv (a). (B) Quantitative antibody responses of healthy subjects (HS) and different groups of patients (PTB, DTB, RTB, TtTB, LP) to culture filtrate proteins of M. tuberculosis (I-VII). Solid lines represent cut-off value decided by ROC analysis. CI, clinical isolates.](/content/175/2012/135/5/img/IJMR-135-745-g001.png)
-
(A): Scatter diagram of IgG antibody response to whole cell extract from various selected clinical isolates with individual serum from different groups of patients [patients with fresh pulmonary tuberculosis (PTB), defaulter TB (DTB), relapse TB (RTB), treated TB (TtTB), and lepromatous leprosy patients (LP)] and controls (HS, healthy subjects) (b-l) in comparison with M. tuberculosis H37Rv (a). (B) Quantitative antibody responses of healthy subjects (HS) and different groups of patients (PTB, DTB, RTB, TtTB, LP) to culture filtrate proteins of M. tuberculosis (I-VII). Solid lines represent cut-off value decided by ROC analysis. CI, clinical isolates.
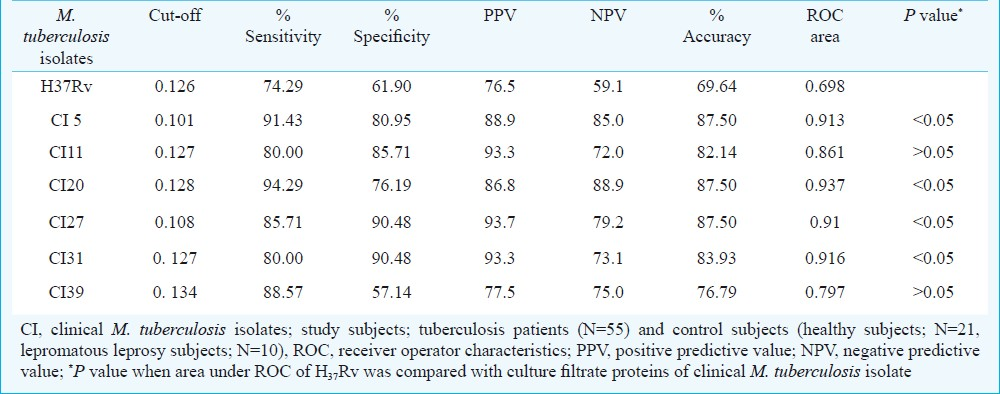
Antibody response to CFP collected at different time points (7, 14, 21, 28 and 35 days) from 11 selected clinical isolates of M. tuberculosis was analyzed by ELISA taking a panel of pooled serum samples from patients with various categories of tuberculosis and controls. Highest antibody levels were observed against 21 and 35 days culture filtrate. A total six culture filtrates from clinical isolates (CI5, 11, 20, 27, 31 and 39) which showed higher antibody (> 2 times than controls) to pooled serum of different categories of tuberculosis patients were selected for further analysis using different individual serum (Fig. 1B). Antibody reactivity to four culture filtrate of clinical isolates (CI5, CI20, CI27 and CI31) was significantly (<0.05) higher as compared with H37Rv (Table II). Most of the CFP of clinical isolates (CI5, CI20, CI27 and CI39) as well as H37Rv showed strong reactivity to PTB serum than their WCE. However, low antibody response to PTB was noted to culture filtrate of CI11 and CI31 as compared to their WCE. Defaulter tuberculosis cases (DTB) were also less reactive to CFP in comparison to WCE to four clinical M. tuberculosis isolates (CI11, CI27, CI31 and CI39) and H37Rv (Fig. 1 A and B). Similar reactivity of CFP to relapsed TB cases (RTB) was noted (CI5, CI20 and CI39) and lower (CI11 and CI31) than their WCE. Only CFP of CI27 was showing high reactivity to RTB than WCE. The reactivity of treated tuberculosis patients (TtTB) against CI5 and 39 was higher than WCE of similar isolates. Lepromatous leprosy patients’ serum was less reactive to CFP of all clinical isolates (CI5, 11, 20, 31 and 39) as well as to H37Rv except CI27 as compared with their corresponding WCE. Accuracy of all CFP was comparatively higher than H37Rv using cut-off determined by ROC analysis (Table II). These CFP of clinical M. tuberculosis isolates belonged to prevalent genotypes; CI5, CAS1_Del (ST-26); CI11, CAS1_Del (ST-26); CI20, CAS1_Del (ST-26); CI27, East African Indian (ST-11); CI31, Beijing family (ST-1) and CI39, CAS1_Del (ST-26) family.
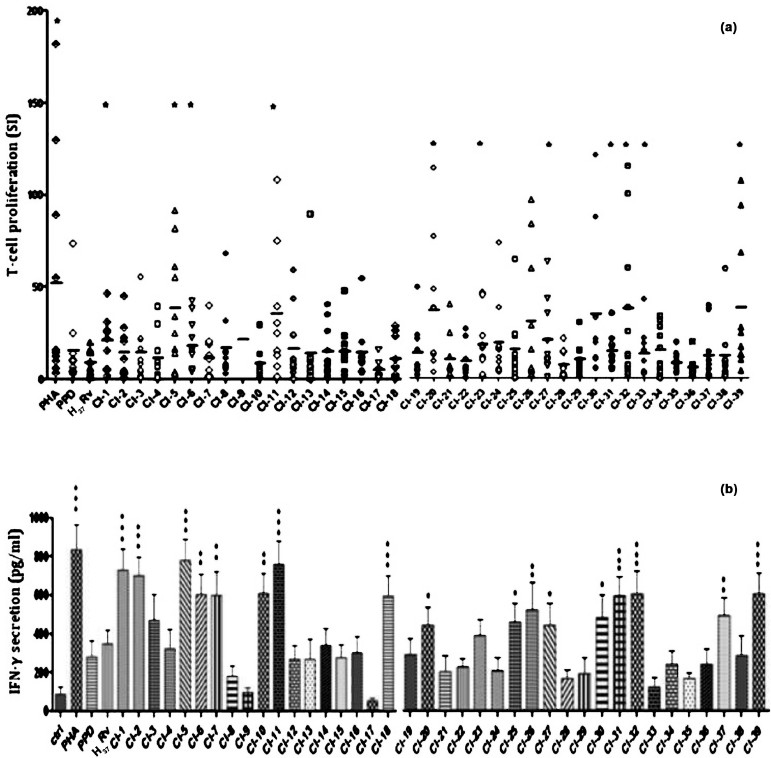
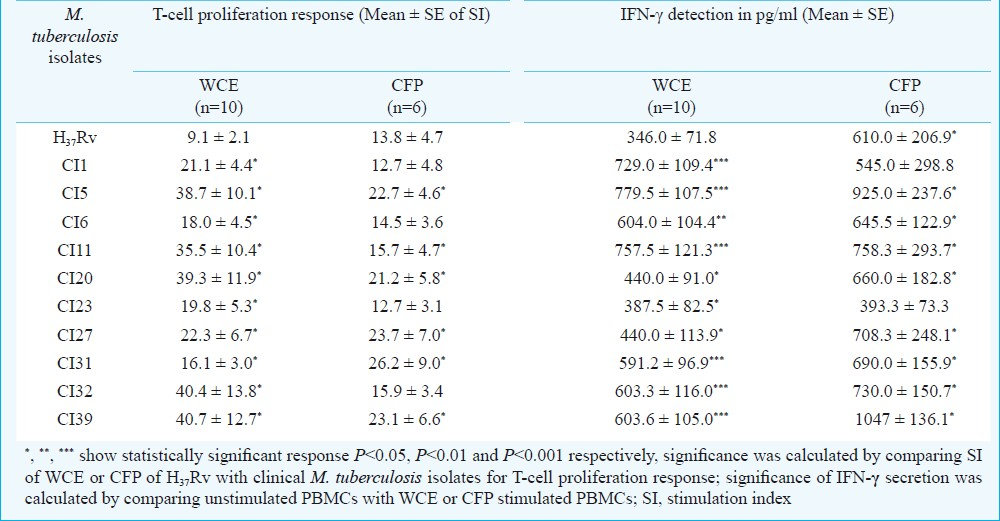
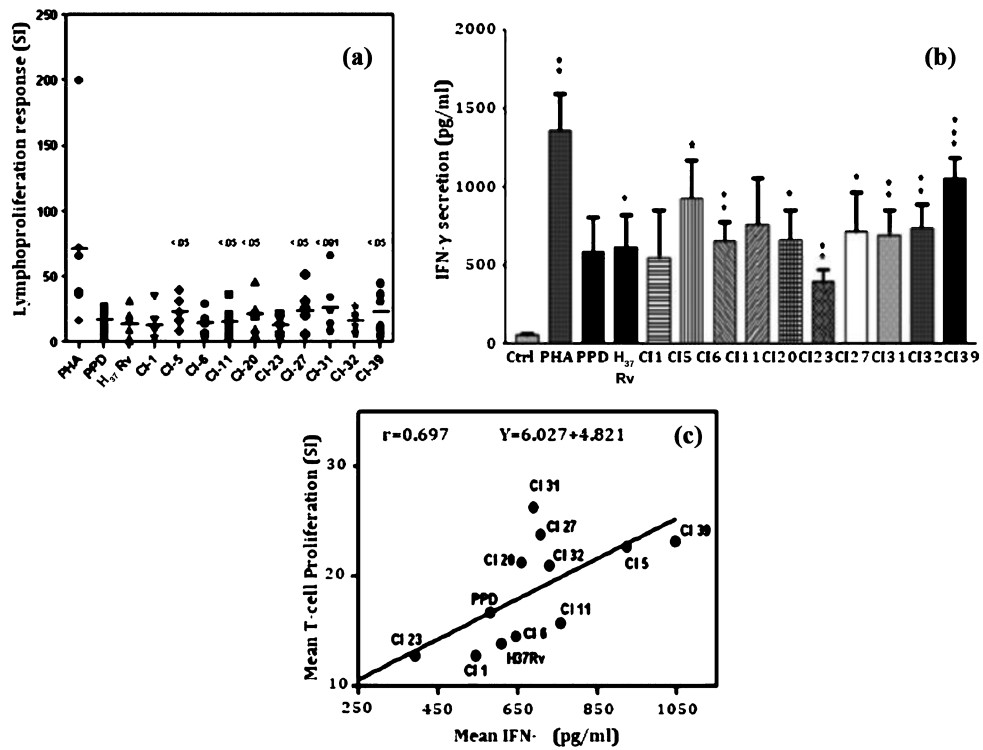
Cell mediated immune response of whole cell extracted and culture filtrate proteins: The WCE of CI1, 5, 6, 11, 20, 23, 27, 31, 32 and 39 induced significantly higher levels of T-cell proliferation as compared to H37Rv and IFN-γ secretion as compared to unstimulated PBMCs (fig. 2a, 2b and Table III) but IL-4 levels was not significantly higher for any WCE of clinical isolate as well as for H37Rv as compared to unstimulated PBMCs (data not shown). The relative efficacies of CFP preparations from 10 selected clinical isolates of M. tuberculosis were also analyzed by stimulating PBMCs from healthy donors. A comparison of the different CFP preparations revealed that the CFP of CI5, 11, 20, 27, 31, 32 and 39 clinical isolates were statistically more potent in inducing cell proliferation than those of H37Rv and PPD (P<0.05 for CI5, 11, 20, 27, 39 and <0.001 for CI31) (Fig. 3a). CFP preparations of clinical isolates which were significant inducers of T-cell proliferation were also the potent stimulator of IFN-γ secretion by PBMCs (Fig. 3b and 3c). Responses to different CFP preparations indicated that the CFPs derived from CI39 induced maximum IFN-γ, which was significantly higher (P <0.001) than the response to CFPs of H37Rv and PPD (Fig. 3b). IL-4 concentration was also determined in culture supernatants of PBMCs stimulated with or without CFPs (data not shown). A moderate increase in IL-4 secretion was induced only by some CFPs (CI5, CI32 and CI39). The relative efficacy of different CFP preparations to induce T-cell proliferation and IFN-γ secretion were not similar for all PBMC preparations. Efficacy of different CFP preparations from clinical isolates in proliferation and IFN-γ assays were correlated and a positive correlation between the two parameters of T-cell activation was observed for clinical isolates (r, 0.697; Fig. 3c).
-
(a): T-cell proliferation response and (b) IFN-γ levels secreted by PBMCs of healthy individuals induced by whole cell extracts from 39 clinical M. tuberculosis isolates (CI), H37Rv, PPD standard, and Mitogen phytohemagglutinin (PHA); Ctrl, unstimulated PBMC, Bar represents the mean value of stimulation index (SI) for each isolate. Statistical significance of T-cell proliferation response was calculated using paired t-test by comparing the stimulation index values of H37Rv and clinical isolates, P value for IFN-γ secretion was calculated by comparing unstimulated PBMCs (Ctrl) with WCE or CFP stimulated PBMCs, *P<0.05, **P<0.01, ***P<0.001.
-
(a): Lymphoproliferation response of PBMCs derived from healthy individuals to culture filtrate proteins of clinical isolates, M. tuberculosis strain H37Rv, standard PPD and Mitogen phytohemagglutinin (PHA). Results are expressed as stimulation index (SI) and statistical significance was calculated using paired t-test by comparing the stimulation index values of H37Rv and clinical isolates, CI; clinical isolates of M. tuberculosis; bar represents the mean value of SI.
-
(b). Cytokine IFN-γ secretion from PBMCs of healthy individuals following stimulation with culture filtrate protein preparations of clinical isolates, H37Rv, PPD and PHA. Bars represent means±standard errors of the means. CI; clinical isolates of M. tuberculosis.Statistical comparison between unstimulated and stimulated cells was performed using the paired t-test. *P<0.05.
-
(c). Correlation of efficacies of different CFP preparations for T-cell proliferation and IFN-γ secretion assays. Mean for all culture filtrate protein (CFP) preparations in T-cell proliferation and IFN-γ secretion assays were determined and plotted against each other and Spearman correlation coefficient (r) is calculated. Y intercept is calculated taking X intercept=0.0.
Discussion
Immune response of host could be a good indicator of exposure to M. tuberculosis. Failure of BCG in TB endemic countries is the major bottleneck for the control of this disease. Therefore, exhaustive research is going on to find new candidate antigens for the diagnosis and vaccine for TB. Most of the studies have been conducted on the purified antigens of laboratory strain H37Rv which has been passaged over the years and might have lost some of the immunodominant antigens. It is possible that most recent and prevalent strains of M. tuberculosis could induce more specific and dominant immune response and characterization of these antigens could lead to identification of some new antigens. The present study was therefore undertaken to evaluate antibody response, lymphoproliferative, IFN-γ and IL-4 responses of PPD positive healthy individuals and TB patients to clinical isolates of M. tuberculosis belonging to different geographical regions of India. Significantly higher antibody reactivity was noted in TB patients with WCE of certain clinical isolates than H37Rv. Most of the culture filtrates of clinical isolates were strongly reactive with fresh pulmonary TB cases in comparison to WCE of same isolate. In contrast, the reactivity to relapsed (RTB) and defaulter TB (DTB) cases was lower to culture filtrate than whole cell extracts of most of clinical isolates. This was a preliminary approach to find out immunologically relevant clinical isolates, as the cases of relapsed TB (RTB), defaulter TB (DTB) and lepromatous (LL) leprosy groups used in the present study were not sufficient to make a valid conclusion. Serum samples from leprosy patients showed strong antibody response to all clinical isolates. It appears that the immunodominant cross-reactive antigens of M. leprae are expressed in clinical M. tuberculosis isolates, some of which antigens are not expressed in H37Rv. Further, reactivity of leprosy patients’ serum samples against culture filtrate of most of the clinical isolates was less than that observed for whole cell extract. This finding suggests that M. tuberculosis secretes more specific molecules in culture medium.
Correlation of T-cell proliferation and IFN-γ secretion parameters with protective immunity has been shown1718. In our study, T cell lymphoproliferative response and IFN-γ production of healthy individuals after stimulation with whole cell extracts of clinical isolates were significantly higher than the response with standard laboratory strain H37Rv. Whole cell extracts of certain clinical isolates showed good correlation of antibody reactivity, lymphoproliferative response and IFN-γ production suggesting that these isolates could have promising molecules for immune based detection of tuberculosis and immune intervention. A study conducted in southern India also evaluated the potential of sonicated antigens from highly prevalent strains from south India in induction of protective immunity and humoral response19.
M. tuberculosis isolates used in this study were cultured and harvested under the same standard culture conditions to minimize the differences in protein expression2021. Various studies have demonstrated that antigens present in culture filtrate (CF) are inducers of protective immunity in mice and humans with TB2223. Therefore, antibody, LTT and IFN-γ response of TB patients and healthy individuals to CF of clinical isolates was analyzed. High percentage of accuracy was noted for all six culture filtrates of clinical isolates than H37Rv when antibody response was analyzed. Four out of five healthy individuals showed good proliferation response to culture filtrate of all clinical isolates whereas three healthy individuals showed good response to H37Rv. CF of most of the clinical isolates induced higher IFN-γ than H37Rv. IL-4 production was not significant, however in three isolates the culture filtrates induced moderately higher IL-4 response in most of the healthy individuals than that induced by H37Rv suggesting both Th1/Th2 inducing nature of culture filtrate of these isolates. Siddiqui et al have also evaluated T cell proliferation, IFN-γ and IL-12 secretion against CF from six isolates of M. tuberculosis and found similar results as ours24. It has been shown that different M. tuberculosis isolates elicit different Th1 type immune response during the early phase of infection using mice model25, as well as different levels of virulence26. It is interesting that immunologically relevant six culture filtrates identified in the present study belonged to prevalent genotypes [Central Asian Strain CAS1_Del (ST-26), East African-Indian (ST-11) and Beijing family (ST-1)] of M. tuberculosis. CAS1_ Del, East African Indian families of M. tuberculosis isolates are of particular interest to provide insights into regional TB epidemiology because these are the most prevalent strains in Northern and other parts of India as defined by previous studies27–31.
In conclusion, culture filtrate proteins are early recognized by host cell and, therefore, important for signaling pathways. Strong immune response to culture filtrate proteins extracted from prevalent clinical M. tuberculosis isolates highlighted the presence of immunodominant protein(s) in these clinical isolates that could be in addition to so far identified M. tuberculosis antigens. Therefore, systematic advanced proteomic and immunological profiling of these prevalent clinical M. tuberculosis isolates may lead to identify functional targets for pathogenic mechanisms, diagnosis and prevention of tuberculosis.
Acknowledgment
Authors thank Dr Bharat Bajaj, State TB Demonstration and Training Centre and Dr Rajesh Gupta, S.N. Medical College, Agra for providing clinically diagnosed samples of tuberculosis patients and Dr BK Girdhar, NJIL & OMD (ICMR) for providing well diagnosed serum samples of leprosy patients. This work was financially supported by Department of Biotechnology, New Delhi. The first Author (GK) is Senior Research Fellow of UGC-CSIR, New Delhi. Authors also thank Shriyut Malikhan Singh Tomar and MM Alam for their technical help.
References
- World Health Organization. In: Global tuberculosis control; surveillance, planning, financing. Geneva: WHO; 2009.
- [Google Scholar]
- Cross-reactive immunity to Mycobacterium tuberculosis DosR regulon encoded antigens in individuals infected with environmental, non-tuberculous mycobacteria. Infect Immun. 2009;77:5071-9.
- [Google Scholar]
- Delayed type hypersensitivity, mycobacterial vaccines and protective immunity. Lancet. 1994;344:1245-9.
- [Google Scholar]
- Using a label-free proteomic method to identify differentially abundant proteins in closely related hypo- and hyper-virulent clinical Mycobacterium tuberculosis Beijing isolates. Mol Cell Proteomics. 2010;9:2414-23.
- [Google Scholar]
- Strain identification of Mycobacterium tuberculosis by DNA fingerprinting: recommendations for a standardized methodology. J Clin Microbiol. 1993;31:406-9.
- [Google Scholar]
- Simultaneous detection and strain differentiation of Mycobacterium tuberculosis for diagnosis and epidemiology. J Clin Microbiol. 1997;35:907-14.
- [Google Scholar]
- Mycobacterium tuberculosis complex genetic diversity: mining the fourth international spoligotyping database (SpolDB4) for classification, population genetics and epidemiology. BMC Microbiol. 2006;6:23.
- [Google Scholar]
- Identification Mycobacterium tuberculosis complex strains families using spoligotypes. Infect Genet Evol. 2006;6:491-504.
- [Google Scholar]
- Properties of energy transducing system in different types of membrane preparations from Mycobaterium phlei; preparation, resolution and reconstitution. Methods Enzymol. 1979;55:175-99.
- [Google Scholar]
- A rapid and sensitive method for the quantitative of microgram quantities of protein utilizing the principle of protein dye binding. Anal Biochem. 1976;72:248-54.
- [Google Scholar]
- A simple and rapid method of sample preparation from culture filtrate of Mycobacterium tuberculosis for two-dimensional gel elecrophoresis. Braz J Microbiol. 2010;41:295-9.
- [Google Scholar]
- Revised National Tuberculosis Control Programme (RNTCP) at a Glance. :5. Available from: http://uttarkashi.nic.in/Dept/Health/RNTCP/RNTCP.pdf
- [Google Scholar]
- Diagnostic potential of Ag85C in comparison to various secretory antigens for childhood tuberculosis. Scand J Immunol. 2008;68:177-83.
- [Google Scholar]
- Separation of leukocytes from blood and bone marrow. Scand J Clin Lab Invest. 1968;97(Suppl):7.
- [Google Scholar]
- Disseminated tuberculosis in interferon-γ gene disrupted mice. J Exp Med. 1993;178:2243-7.
- [Google Scholar]
- Induction of in vitro human macrophage anti Mycobacterium tuberculosis activity: requirement for IFN-γ and primed lymphocytes. J Immunol. 1998;160:4490-9.
- [Google Scholar]
- Cell mediated immune response of healthy laboratory volunteers to sconicate antigens prepared from the prevalent strains of Mycobacterium tuberculosis from south India harboring a single copy of IS 6110. Clin Diagn Lab Immunol. 2003;10:1149-52.
- [Google Scholar]
- Hypoxic response of Mycobacterium tuberculosis studied by metabolic labeling and proteome analysis of cellular and extracellular proteins. J Bacteriol. 2002;184:3485-91.
- [Google Scholar]
- Comparative proteome analysis of Mycobacterium tuberculosis grown under aerobic and anaerobic conditions. Microbiology. 2004;150:3821-9.
- [Google Scholar]
- T-cell proliferation responses to antigens secreted by Mycobacterium tuberculosis. Infect Immun. 1991;59:1558-63.
- [Google Scholar]
- Human immune response to Mycobacterium tuberculosis antigens. Infect Immun. 1991;59:665-70.
- [Google Scholar]
- Effect of CFP preparation from Indian isolates of Mycobaterium tuberculosis to activate T-cells derived from healthy donors. Int J Tuberc Lung Dis. 2000;4:980-7.
- [Google Scholar]
- Virulence of a Mycobacterium tuberculosis clinical isolate in mice is determined by failure to induce Th1 type immunity and is associated with induction of IFN-α/β. Proc Natl Acad Sci USA. 2001;98:5752-7.
- [Google Scholar]
- Correlation of virulence, lung pathology, bacterial load and delayed type hypersensitivity responses after infection with different Mycobacterium tuberculosis genotypes in a BALB/c mouse model. Clin Exp Immunol. 2004;137:460-8.
- [Google Scholar]
- Molecular typing of Mycobacterium tuberculosis isolates from a rural area of Kanpur by Spoligotyping and Mycobacterial interspersed repetitive units (MIRUs) typing. Infect Genet Evol. 2008;8:621-6.
- [Google Scholar]
- Predominace of a novel Mycobacterium tuberculosis genotype in the Delhi region of India. Tuberculosis (Edinb). 2002;82:105-12.
- [Google Scholar]
- Predominant tuberculosis spoligotypes, Delhi, India. Emerg Infect Dis. 2004;10:1138-42.
- [Google Scholar]
- Spoligotyping of Mycobacterium tuberculosis isolates from patients with pulmonary tuberculosis in Mumbai, India. Res Microbiol. 2005;156:588-96.
- [Google Scholar]
- rpoB gene sequencing and spoligotyping of multidrug-resistant Mycobacterium tuberculosis isolates from India. Infect Genet Evol. 2006;6:474-83.
- [Google Scholar]




