Translate this page into:
How endemic is cholera in India?
*For correspondence: Dr G.B. Nair, Executive Director, Translational Health Science & Technology Institute, 496 Phase III, Udyog Vihar, Gurgaon 122 016, Haryana, India gbnair_2000@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Cholera continues to remain an important public health concern in developing countries. Globally, the true number of cholera cases is known to be much higher than reported. The discrepancy results from underreporting and other surveillance system limitations, including inconsistencies in case definitions and lack of a standard vocabulary1. The reporting system for cholera lacks standardization as only outbreaks are reported. As per the new definition of endemic cholera given during a meeting of the WHO Strategic Advisory Group of Experts (SAGE) on immunization held in October 2009 in Geneva, the occurrence of faecal culture-confirmed cholera diarrhoea in a population in at least 3 of the past 5 years confirms the area as endemic for cholera2.
As a WHO Collaborating Center for Diarrhoeal Diseases Research and Training, the National Institute of c0 holera and Enteric Diseases (NICED), Kolkata, West Bengal, India, receives about 1000 to 1500 strains of Vibrio cholerae every year from about 30 to 40 institutions from India and a few from outside the country for biotyping, serotyping and phage typing. During 1990-2007, a total of 16,624 strains of Vibrio cholerae were received from 24 States, of which 7,225 strains of V. cholerae were included for phage typing study. All these strains of V. cholerae were identified and confirmed by standard techniques3. Strains were serotyped using polyvalent O1 and monospecific Inaba and Ogawa antisera, and monoclonal antibody O139 (Difco, USA). Phage typing was performed by the standard methodology used at our laboratory45. In the present study, we used the place from where strains of V. cholerae O1 were received from different parts of the country during different years as a proxy measure to determine whether a given area was endemic for cholera.
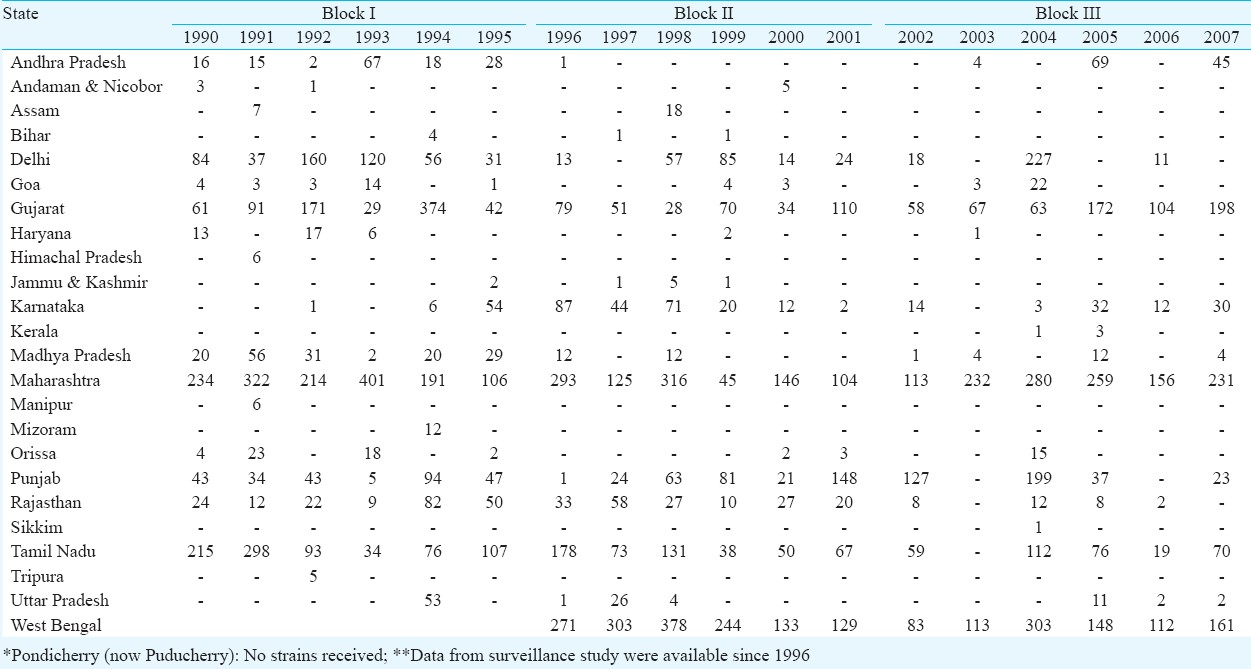
Our results indicated that 11 of the 28 States were endemic for cholera because the disease occurred in three consecutive years in that given area as reflected by culture positive strains sent from that State to our Phage typing Unit (Table). During the study period, 16,624 strains were received at NICED (both O1 and O139). The study period (18 yr) was divided in three time blocks (1990 to 1995-Block I, 1996 to 2001-Block II and 2002 to 2007-Block III). It was found that 24 of the 35 States and union territories sent strains at least once in this period. The States which sent strains in consecutive three years in any block were Andhra Pradesh, Delhi, Goa, Gujarat, Karnataka, Madhya Pradesh, Maharashtra, Punjab, Rajasthan, Tamil Nadu and West Bengal. Highest number of strains were received from Maharashtra, followed by West Bengal, and the pathogen was isolated every year during the study period. No strains were submitted from Puducherry in this period. From 2004 onwards, the new States entering in the cholera map were Kerala and Sikkim. Of the total strains received, 96.5 per cent strains were serotyped as Ogawa and the remaining 3.5 per cent were Inaba. Periodic shifts in the occurrence of Ogawa and Inaba serotypes in a given area are usual phenomenon and is thought to be a consequence of population-level immunity patterns6.
All these strains were clustered under type 2 and 4 when phage typed with Basu and Mukerjee scheme7. Almost 100 per cent typeability was observed with the new scheme8 with type 27 being the dominant phage type. On this basis, these strains can be divided in to three groups, T2-T27 (52.5%), T4-T27 (32.8%) and UT-T27 (14.7%), suggesting that three closely related clones were disseminated in India. Our study showed that type 27 was the dominant type in all parts of the country followed by type 26.
Our analysis shows that cholera occurs over a wider geographic area in India than was previously recognized. The annual number of cholera cases reported to WHO by the government was several times lower than the numbers we obtained through strains received at the Phage typing unit. This may be due to lack of surveillance as well as proper laboratory support and, therefore, the burden of cholera in India is clearly underestimated9. Data from population-based diarrhoea surveillance in an endemic area of Kolkata, India, revealed a cholera incidence of 2.2 cases per 1000 person-years10. If one extrapolates these phage data to all endemic areas in the country, the total number of cases would far exceed the numbers quoted above. Our findings also indicate that cholera is an under-recognized problem in India.
References
- World Health Organization. Cholera: Global surveillance summary, 2008. Wky Epidemiol Rec. 2009;84:309-24.
- [Google Scholar]
- World Health Organization. Meeting of the Strategic Advisory Group of Experts on immunization, October 2009-conclusions and recommendations. Wkly Epidemiol Rep. 2009;84:517-32.
- [Google Scholar]
- Distribution of phage type of Vibrio cholerae O1 biotype ElTor in Indian scenario (1991-98) Indian J Med Res. 1999;109:204-7.
- [Google Scholar]
- Detection of virulence associated and regulatory protein genes detection in association with phage typing of human Vibrio cholerae population from several geographical regions of world. J Med Microbiol. 2009;58:1160-7.
- [Google Scholar]
- New phage typing scheme for Vibrio cholerae O1 biotype El Tor strains. J Clin Microbiol. 1993;31:1579-85.
- [Google Scholar]
- The high burden of cholera in children: comparison of incidence from endemic areas in Asia and Africa. PLoS Negl Trop Dis. 2008;20(2):e173.
- [Google Scholar]
- Cholera in India: an analysis of reports, 1997-2006. Bull World Health Organ. 2010;88:185-91.
- [Google Scholar]




