
Translate this page into:
18F FDG PET/CT clearly showed a case of lymphoma involving kidneys & bones without morphological abnormality
* For correspondence: yccbp@126.com
-
Received: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 31 yr old male† presented to the Infectious Diseases Department of Yichang Central People’s Hospital, Hubei province, P.R. China, in June 2017, with a fever of unknown origin for over three weeks. The positive laboratory results mainly included erythrocytopenia (3.62×1012/l; normal range: 4.3-5.8), leukopenia (3.21×109/l; normal range: 3.5-9.5), thrombocytopenia (118×109/l; normal range: 125-350) and a marked increase in the level of lactate dehydrogenase (1208 IU/l; normal range: 120-250).
However, imaging examinations, including non-enhanced chest and abdominal computed tomography (CT) and abdominal ultrasound were unremarkable (Fig. 1). A whole-body 18Fluorine labelled fluorodeoxyglucose positron-emission computed tomography/CT (18F-FDG PET/CT) was done to look for occult infection or malignancy. PET/CT images (Fig. 2) showed abnormally elevated FDG uptake in bilateral kidneys and humerus, left femoral neck and retroperitoneal lymph nodes (all <1 cm in diameter) with a maximum standardized uptake value (SUVmax) of 18.1. No obvious morphological abnormalities were observed in these hypermetabolic lesions on non-enhanced CT. Subsequently, non-Hodgkin’s cytotoxic T-cell lymphoma was confirmed by immunohistochemistry (Fig. 3) through left femoral neck puncture biopsy under the guidance of PET/CT and the patient was transferred from the infectious diseases to the haematology department for treatment. After two cycles of chemotherapy, a repeat PET/CT revealed that the metabolic activity returned to the normal level with a SUVmax of 3.0 (Fig. 4).
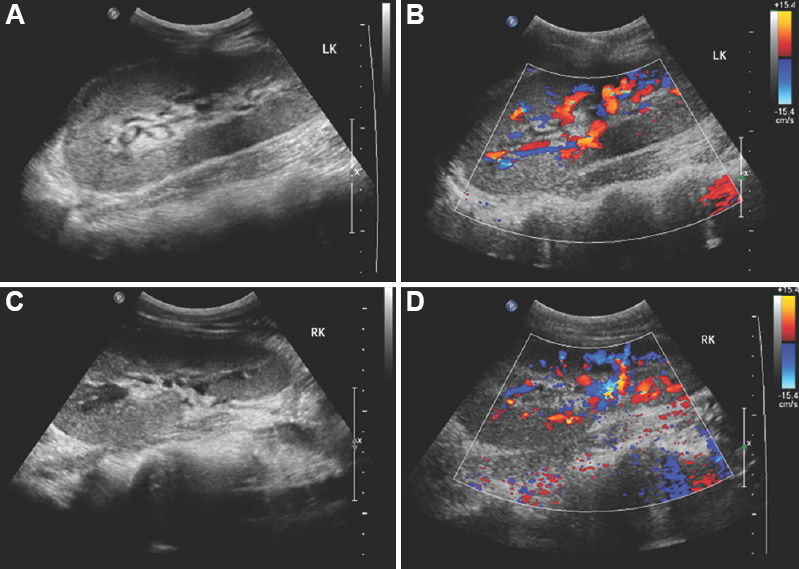
- Renal ultrasound before treatment indicated that there were no obvious abnormalities in the size, shape and sonographic manifestations of both kidneys. Panel A and B show the left kidney and C and D represent the right kidney.
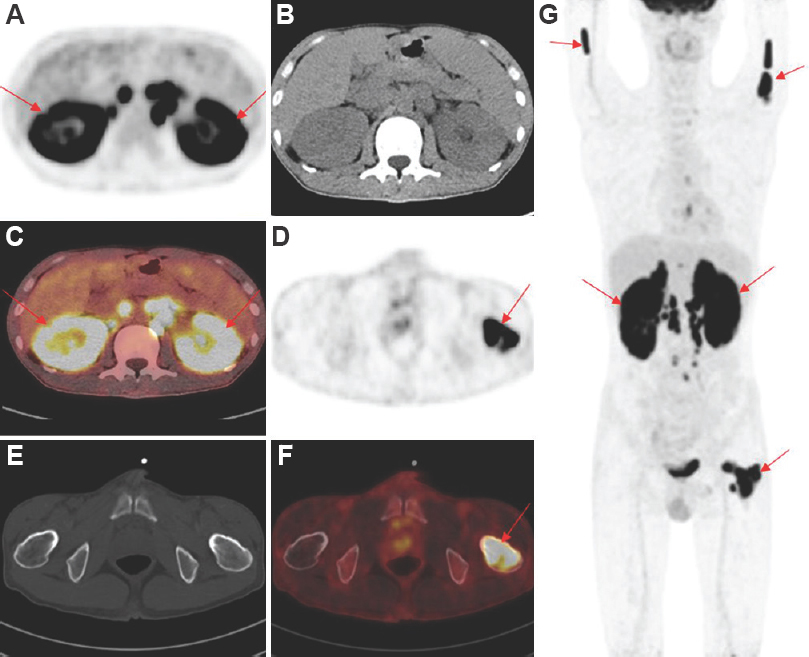
- PET/CT images before chemotherapy. Panel A-C show renal PET, CT and PET/CT fusion images, respectively. Panel D-F show PET, CT and fused PET/CT images of the left femoral neck, respectively. (G) MIP image shows abnormal FDG uptake in the bilateral kidneys and humerus, left femoral neck and retroperitoneal lymph nodes. The SUVmax of kidney and bone lesions were 18.1 and 17.0, respectively. Arrows indicate lesions. FDG PET/CT, flurodeoxyglucose positron-emission computed tomography, MIP, maximum intensity projection; SUVmax, maximum standardized uptake value.
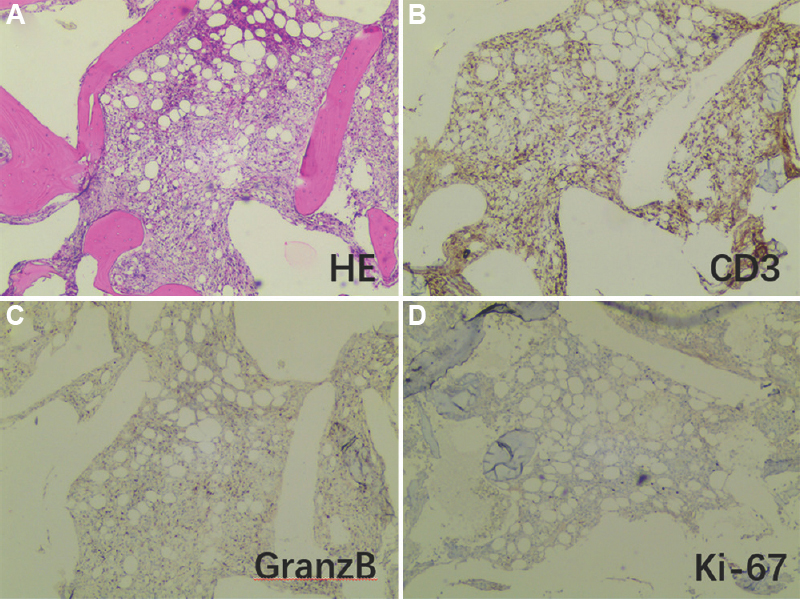
- The left femur neck lesion biopsy under the guidance of PET/CT. (A) Haematoxylin and eosin staining showing normal bone marrow structural destruction, with small remnants of adipose tissue and proliferating fibrous connective tissue and atypical lymphocyte infiltration. Immunohistochemical results: (B) MPO (−), CD235 (erythrocyte +), CD61 (−), CD3 (+), (C) CD20 (−), GranzB (scattered +), (D) ki-67 (hot spot LI about 20%+), CD56 (−), CD30 (−), ALK(ALK1), CD138 (−), EBER-CISH (−). Combined with clinical data, it was considered that non-Hodgkin’s cytotoxic T-cell lymphoma involves bone marrow. (A-D, ×20).
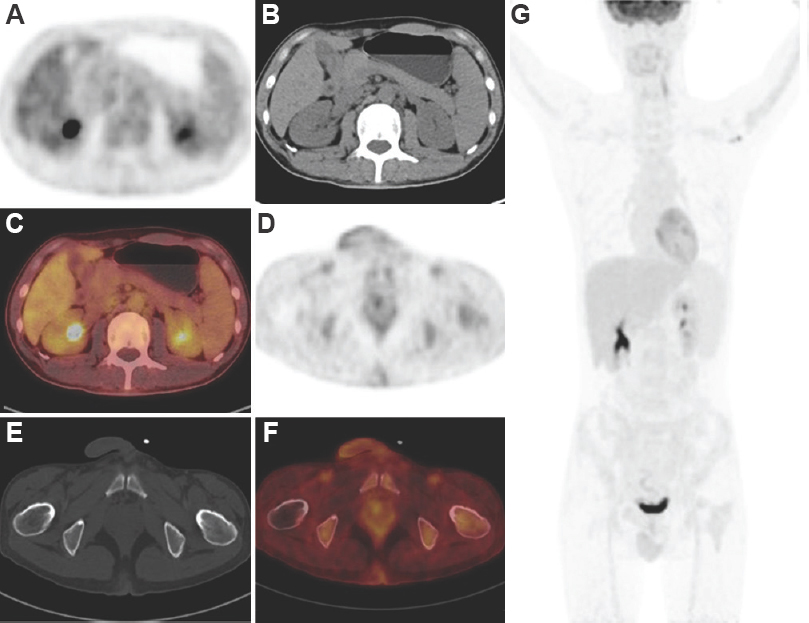
- After two cycles of chemotherapy, a repeat PET/CT showed that all previous hypermetabolic lesions disappeared. Panel A-C showed PET, CT, and PET/CT fusion images of both kidneys, respectively. Panel D-F showed PET, CT and PET/CT fusion images of the left femoral neck, respectively. (G) displayed MIP image of the whole body.
Lymphoma can involve a variety of tissues and organs outside the lymph nodes. When there is no obvious morphological abnormality, traditional imaging may not pick up abnormal lesions. However, an 18F-FDG PET/CT can be invaluable in diagnosing an occult malignancy and for subsequent evaluation for the remission of disease.
Acknowledgment: The authors would like to thank pathology expert Yu-fei Liu, haematology expert Jing-ming Guo and oncology expert Xin-hua Xu, The First Clinical Medical College of Three Gorges University, Yichang, China, for providing professional advice.
Conflicts of Interest: None.




